Foot Pathology: Tarsal Coalition
Tarsal coalition can be congenital or may arise secondarily following surgery, infection, trauma or other joint-space disease. The two most common type of tarsal coalition are calcaneonavicular and talocalcaneal, compromising 90% of cases with nearly equal frequency of occurrence. Patients may be asymptomatic, but often present with foot and ankle pain. Pain is more likely if the coalition is ossified, and the onset of pain is often following minor trauma. Peroneal spastic or rigid flatfoot can accompany tarsal coalition.
If suspected, imaging begins with conventional radiographs. Three views of the foot are necessary, as the oblique view is best for detecting calcaneonavicular and talonavicular coalitions. However, talocalcaneal coalitions are not as reliably diagnosed with conventional radiographs, and often require CT or MRI to detect. CT is helpful in any type of coalition to elucidate whether the union is osseous, fibrous or cartilaginous, to detect secondary OA, and for preoperative determination of the extent of joint involvement and the appropriate type of surgical treatment. Postoperatively, CT can confirm whether a coalition has recurred or detect secondary osteoarthritis.
Calcaneonavicular coalitions are generally seen on 45 degree oblique conventional radiographs. An osseous bar between the calcaneus and navicular may be evident, or the two bones may be in close proximity. A secondary sign is hypoplasia of the talar head (4). The axial orientation is the best plane with which to evaluate calcaneonavicular coalitions using CT. Again, if the coalition is not entirely bony, the primary finding may be a narrowing of the space between the 2 bones.
Talocalcaneal coalitions may not be apparent on oblique conventional radiographs, and MDCT is an excellent modality with which to evaluate the foot if this suspected. The narrow collimation of MDCT and the high quality 3D reconstructions are helpful in evaluating these coalitions with high resolution datasets, which can be viewed in any orientation. This is particularly helpful for detecting talocalcaneal coalitions, which are best visualized in the coronal plane. With MDCT, the high resolution multiplanar reconstructions preclude the requirement for direct coronal acquisitions. These unions usually join the middle facet of the talus to the sustentaculum tali of the calcaneus. An osseous bridge will be apparent if the union is bony. In cartilaginous coalitions, the middle facet joint is markedly narrowed with cortical irregularity. Fibrous coalitions demonstrate slight narrowing of the middle facet joint, and were the most difficult to detect in one series with surgical correlation.
A number of secondary findings have been described using conventional radiographs to detect talocalcaneal coalitions. These include a talar beak at the insertion of the talonavicular ligament, a narrowed posterior subtalar joint, the inability to visualize the middle subtalar joint on the lateral film, broadening of the lateral process of the talus, narrowing of the posterior subtalar joint, among other findings. In addition, Lateur described the “C sign”. This is a reverted C visible along the posterior foot, from the talar dome (superior to posterior), along the posterior talocalcaneal joint, to the sustentaculum tali (inferiorly). This was previously believed to be a reliable sign on conventional radiography, evident in 87-98% of lateral radiographs in the setting of talocalcaneal coalition. Recently, lateral radiographs were correlated with CT and surgery to determine the sensitivity and specificity of this sign. This new data revealed that the “C sign” is only 49% sensitive, but 91% specific for talocalcaneal coalition. One additional finding associated with this type of coalition, irregularity of the posterior talocalcaneal joint, was shown to be 71% sensitive and 93% specific for talocalcaneal coalition. The authors concluded that the C sign was only reliable if the coalition was large or the bones were mature . This new data supports the importance of MDCT if the diagnosis is suspected but the conventional radiograph does not depict the coalition.
Specific imaging findings have been shown to correlate with the outcome of a talocalcaneal coalition and can be used to determine whether the treatment should be resection or immobilization. CT can be used to measure the coalition area and detect osteoarthritis. Resection is indicated if the area is less than 50% of the surface area of the talocalcaneal joint and if secondary degenerative osteoarthritis is not detected in the talonavicular joint.
 |  | |||
Diagnosis: Calcaneonavicular coalition with congenitally short 3rd and 4th digits. | ||||
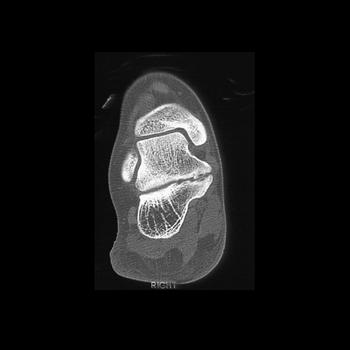 |  | 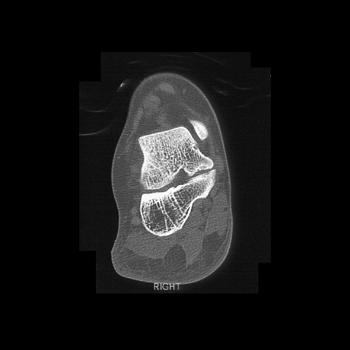 |  | |
Clinical History: 17 year old woman with foot pain. CT Findings: Fibrous coalition of the medial fact of the subtalar joint. Diagnosis: Talocalcaneal coalition. Outcome: Initially opted for observation. | ||||
 |  |  | 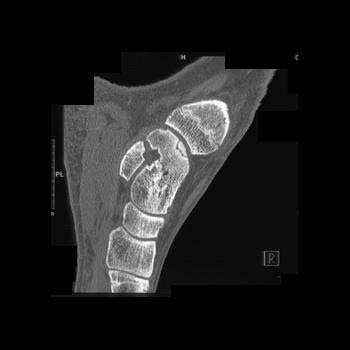 | |
Clinical History: 14 year old boy with 1 year history of right foot pain.The pain is aggravated by playing sports. CT Findings: Nondisplaced osteochondral fragment of the right medial talar dome. Diagnosis: Osteochondral defect medial right talar dome, nondisplaced. The patient did have evidence of avascular necrosis of the talus. | ||||