Foot Pathology: Gout
Gout is one type of arthritis that has a lower extremity predilection. Specifically, the feet are affected in 85% of patients, as well as hands, wrists, elbows and knees. Acute gout is typically a monoarticular or oligoarticular process, generally without any bony changes on radiographs. Gout also has an interval or intercritical phase. This is followed by chronic tophaceous gout, when radiographic changes are more commonly present. Chronic tophaceous gout is more common in men, and often affects women following menopause.
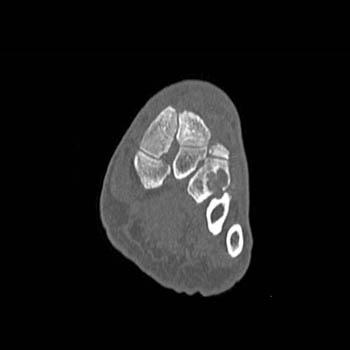
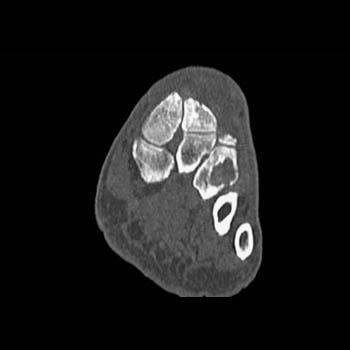
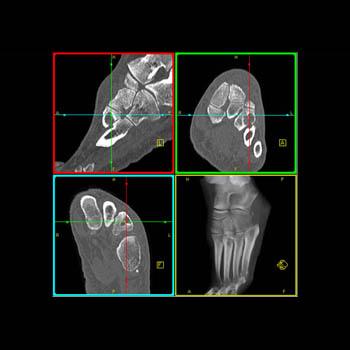
In the feet, gout often involves the 1st metatarsal-phalangeal joint and intertarsal joints (Figure: Gout of the foot). The medial and dorsal surfaces of the 1st metatarsal head are classically affected. Erosions are seen both intraarticular and juxtaarticular, as well as removed from the joint space. These are frequently eccentric with sclerotic borders. The overhanging edge of gouty erosions should be distinguished from the osteophytes of OA, and unlike OA, the joint space is usually well preserved until late in the course of gout . Any metatarsal phalangeal joint can be involved, particularly the 5th, and interphalangeal joints can also be affected. Lysis of the phalanges can result in nonvisualization, and secondary fractures can complicate the picture.
Periarticular soft tissue masses represent tophaceous deposits of chronic gout, which can also be seen in the subcutaneous region and tendon. Studies using conventional radiographs reported that tophi are uncalcified; however, recent MR and CT studies reveal that cross sectional imaging will demonstrate calcification within tophi. The calcification is often stippled, or can be sheet-like.
The calcaneus can be affected by gout, with erosion and retrocalcaneal bursitis. Gout can cause enlargement and even rupture of the Achilles tendon. Attention should be paid to this region when performing CT or MRI of the foot in the setting of gout.
 |  |  |  |
 |  |  |  |
Diagnosis: Spitfire gout. | |||