Foot Pathology: Diabetes
The diabetic foot is afflicted by a number of different pathologies, including infection, neuropathic osteoarthropathy and vascular disease. In many cases, the exact etiology of bony abnormalities and clinical symptoms is difficult to determine and may be multifactorial. A combination of imaging may be necessary for diagnosis and determination of extent of pathology, including MR, CT and nuclear medicine. CT is primarily used in the evaluation of infection and neuropathic osteoarthropathy. Infection was reviewed above, so neuropathic osteoarthritis will be discussed.
Neuropathic arthropathy often coexists with infection in the midfoot and forefoot of diabetics. The deterioration of sensation and proprioception result in recurrent foot injuries. In the diabetic, this is aggravated by the other coexisting diseases of ischemia and infection. Although diabetes is the most common cause of neuropathic osteoarthropathy, neuropathic osteoarthropathy afflicts only a small percentage of diabetics.
The regions of the foot that are most prone to neuropathic arthropathy include the forefoot, the metatarsal-phalangeal joints, the tarsal-metatarsal joints and intertarsal joints.
Neuropathic osteoarthropathy begins with an acute, resorptive, hyperemic phase. On imaging studies, the bone abnormalities are similar in appearance to infection. The forefoot is involved most commonly, followed by the midfoot. The metatarsal-phalangeal joint regions may demonstrate osteolysis.
The sclerotic or hypertrophic stage follows. Bone abnormalities include sclerosis, erosions, fractures with fragmentation, joint dissolution and subluxation or dislocation resulting in malalignment (Figure here: Charcot Joint).
The definitive determination of whether bone changes in the diabetic foot are due to infection or neuropathic osteoarthropathy may require a combination of cross sectional imaging and nuclear medicine. Berquist described some features more consistent with one diagnosis or the other. Neuropathic disease should be suspected in the midfoot, if the distribution is polyarticular, in the absence of cortical lesions and if the bone abnormality is located at a distance from the skin ulcer or soft tissue infection. Alternatively, infection should be considered if the bone changes are in close proximity to a skin ulcer or soft tissue infection, if the toes and/or metatarsal heads are involved and if cortical erosions are detected.
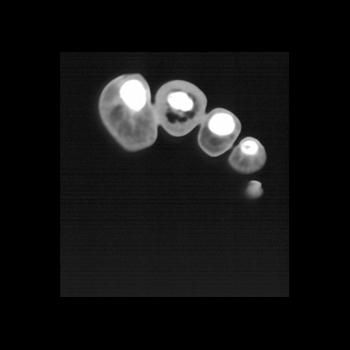 | 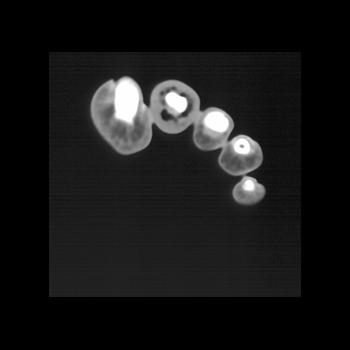 | 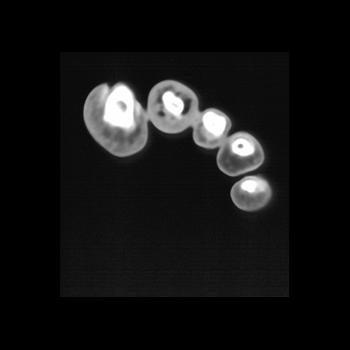 | 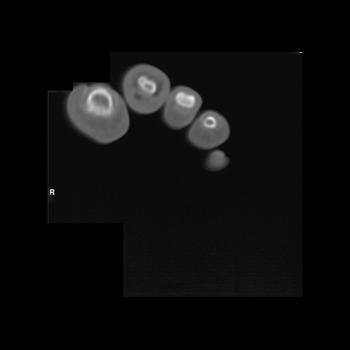 | |
Clinical History: 60 year old man with diabetes and multiple infections with ulceration of the left 2nd toe. He presented to the emergency room with a swollen toe. Plain film radiograph demonstrated air in the distal left second toe. CT Findings: CT demonstrated soft tissue swelling as well as air in the subcutaneous tissues by the 2nd digit. Diagnosis: The CT findings were consistent with the pathologic diagnosis which was gas gangrene. Outcome: The patient underwent amputation of the digit with subsequent skin grafting. | ||||
 |  |  |  | |
Clinical History: The patient has persistent left ankle pain. The patient also has a history of HIV and hepatitis and poorly controlled diabetes. CT Findings: The study demonstrates destruction of the joint space with remodeling of distal tibia and calcaneus. The pattern of the ankle is most consistent with inflammation in the joint space which is secondary in part related to infection. Diagnosis: Many of the changes are related to a Charcot joint. | ||||