- 2
- ,
- 2
- 4
- 6
To Quiz Yourself: Select OFF by clicking the button to hide the diagnosis & additional resources under the case.
Quick Browser: Select ON by clicking the button to hide the additional resources for faster case review.
CASE NUMBER
130





Diagnosis
Moyamoya Secondary to Sickle Cell Disease
Note
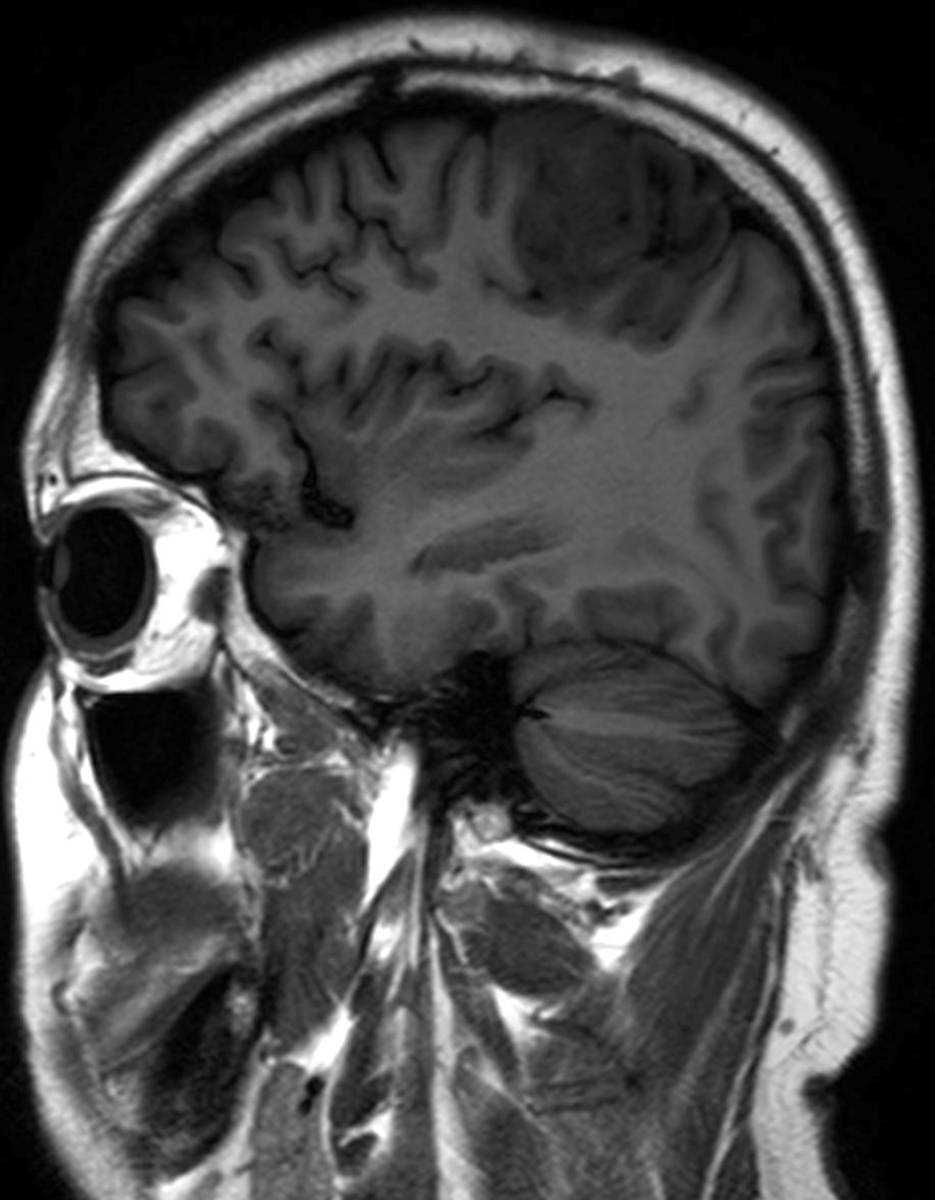
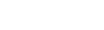
In this 36-year-old female with a history of sickle cell disease, the first image, an ADC map, demonstrates focal regions of diffusion restriction compatible with acute infarcts in the subcortical and deep white matter of the left frontal and parietal regions. The arterial spin label perfusion images, images 2 and 3, demonstrate regions of decreased perfusion, discrepent with the corresponding ADC map representing the presence of an ischemic penumbra, in the right frontal region, left frontoparietal region, and and left cerebellar hemisphere. On the postcontrast axial T1-weighted sequence centered at the level of the Circle of Willis, image 4, a normal appearing left internal carotid terminus is not visualized. Instead, a tangle of vessels is identified extending along the first segments of the anterior and middle cerebral arteries on the left. These findings are confirmed on the coronal postcontrast T1-weighted sequence, image 5. This patient had a prior history of multifocal cerebral infarctions in the setting of sickle cell disease. These images confirm a disgnosis of Moyamoya disease along the left anterior and middle cerebral artery territories. These findings are confirmed on the MR angiography MIP reconstruction, image 6. Moyamoya disease is a result of progressive stenosis and then occlusion of the distal internal carotid arteries and their proximal first-order branches. Extensive collaterals develop at the level of the stenosis and occlusion and may result from dural vessels, leptomeningeal collaterals, and deep perforating lenticulostriate arteries, as in this case. Moyamoya is classically described as a hazy-like puff of smoke on diagnostic angiography.
Related videos to the case