Imaging Pearls ❯ Kidney ❯ Ureter
|
-- OR -- |
|
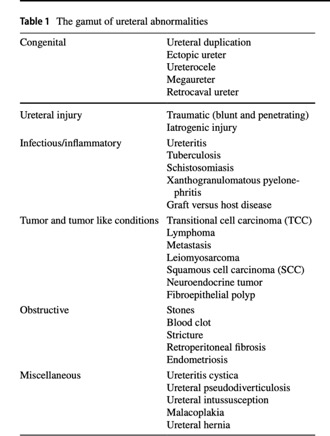
Imaging of ureter: a primer for the emergency radiologist
Mohd Zahid et al.
Emergency Radiology (in press)- “The most commonly used single bolus CT urography protocol includes precontrast scan, nephrographic phase (at 100 s after 100–125 ml intravenous (IV) contrast injection), and delayed excretory phase at 5–20 minutes.”
Imaging of ureter: a primer for the emergency radiologist
Mohd Zahid et al.
Emergency Radiology (in press) - “Ureteral duplication is the most common congenital ureteral abnormality, affecting up to 1% of the population. Duplication can be partial/incomplete or complete, and unilateral or bilateral, with partial duplication being more common. In partial duplication, separate ureters of the upper and lower poles fuse together after a variable distance from the kidney and insert as a single ureter into the urinary bladder. Uretero-ureteral reflux (also known as yo-yo, seesaw, or saddle reflux) is a common but transitory phenomenon. Uretero-ureteral reflux prevents the upper pole moiety from being completely empty and should be suspected when there is asymmetry of the ureters. It results in urine stasis and increased frequency of urinary tract infection . Partial duplication may be associated with pelviureterical junction obstruction of the lower pole resulting in urine stasis, infection, and decrease in the renal excretory func- tion. Uncommonly, it may simulate a renal mass.”
Imaging of ureter: a primer for the emergency radiologist
Mohd Zahid et al.
Emergency Radiology (in press) - "Ureterocele is defined as cystic dilatation of the intramural portion of the distal ureter which appears as a filling defect projecting into the urinary bladder lumen. The inci- dence of ureterocele is 1:5000–12,000 and is 4–7 times more common in females. Ureterocele is subdivided based on location. Intravesical or orthotopic ureterocele occurs when confined within the urinary bladder lumen accounting for 25% of cases and almost always occurring in adults. Ectopic ureterocele extends beyond trigone or outside the bladder and accounts for 75% of cases.”
Imaging of ureter: a primer for the emergency radiologist
Mohd Zahid et al.
Emergency Radiology (in press) - "CT urography is the modality of choice to diagnose ret- rocaval ureter. IVC is seen lateral to the right pedicle of L3 vertebra in 96% of patients with retrocaval ureter, in contrast to 6% of normal people. Therefore, it is the pathognomonic feature of retrocaval ureter. MR urogram is equally effective as CT urography in diagnosing retrocaval ureter. It has advantage of being radiation free modality and also can be performed in patients with poor renal function, during pregnancy, or in pediatric patients. Open surgical ureteroureterostomy is considered as a gold standard surgical intervention.”
Imaging of ureter: a primer for the emergency radiologist
Mohd Zahid et al.
Emergency Radiology (in press) - "Genitourinary tuberculosis is the second most common form of extrapulmonary tuberculosis and usually caused by hematogenous dissemination. It accounts for 15–20% of all extrapulmonary tuberculosis cases. Genitourinary tuberculosis involves the ureter in approximately 50% of the cases. In early disease, IVU or retrograde urography shows ragged and dilated ureter and occasional filling defects of mucosal granulomas. CT urography demonstrates ureteral mural thickening with periureteral inflammatory changes. Tuberculosis tends to involve distal third of the ureter and causes multiple strictures and fibrotic changes with disease progression resulting in a characteristic “beaded or corkscrew” appearance. Chronic mural thickening of the ureter results in foreshortening and “pipestem” ureter. Tuberculosis may also present as pseudotumor due to inflammatory ureteral mural thickening and would be dif- ficult to distinguish from malignancy on imaging. In a small number of cases, ureteral calcifications can be seen.”
- "Schistosomiasis is the most common cause of urinary bladder wall calcification in the endemic nations [80]. Calcification begins at the bladder base which later progresses to circumferential pattern with involvement of entire bladder wall. Circumferential urinary bladder wall calcification resembles “fetal head” on plain radiograph or “shell-like” rim of calcification with reduced capacity on CT. The closest differential of bladder wall calcification is tuberculosis. Linear or parallel linear calcifications of ureters are initially seen in distal ureters, which may progress cranially.”
Imaging of ureter: a primer for the emergency radiologist
Mohd Zahid et al.
Emergency Radiology (in press) - "TCC is the most common urothelial malignancy. The urinary bladder is the most common site, and the renal pelvis is the second most common site. TCC is uncommon in the ureter. TCC occurs in upper urinary tract approximately 5 to 10% of the time, and only 25% of upper urinary tract TCC involves the ureter with the distal one-third ureter being the most common site. TCC constitutes approximately 1% of upper urinary tract malignancies. Synchronous bilateral ureteral TCC occurs in 2–9% of cases. Approximately 11–13% cases develop metachronous upper urinary tract TCC with a mean disease-free interval of 28 months. Metachronous tumor develops in the urinary bladder in 50% of cases of ureteral TCC within 24 months of post-surgical treatment.”
Imaging of ureter: a primer for the emergency radiologist
Mohd Zahid et al.
Emergency Radiology (in press) - "Approximately 15% of ureteral TCC presents with radiological evidence of extramural tumor spread. The most important risk factors of the disease are age > 60 years, male gender, and smoking. Other risk factors include analgesic abuse, occupational exposure to chemical carcinogens such as industrial dyes and plastic, and prior treatment with cyclophosphamide. Chemical exposure predisposes for multifocal lesions . Patients usually present with microscopic or gross hematuria, flank pain, and weight loss. TCC has different growth patterns—“papillary” appears as a filling defect, while “infiltrating” appears as stenosis/stricture.”
Imaging of ureter: a primer for the emergency radiologist
Mohd Zahid et al.
Emergency Radiology (in press) - "It is extremely rare to have disease metastatic to the ureter from any type of primary malignancy. The most com- mon primary malignancies metastasizing to the ureter are breast, colorectal, stomach, prostate, cervical, and melanoma. Three patterns of ureteral metastasis have been described—(1) transmural involvement, (2) periureteral infiltration, and (3) submucosal nodules. The first two patterns are seen as stricture while the is usually multiple filling defects. The adventitia is the most common layer of the ureteral wall to be involved by metastatic disease, while the mucosa is the least common Clinically, most of the patients are asymptomatic and may present with non-specific flank pain and dysuria.”
- "Retroperitoneal fibrosis represents fibro-inflammatory soft tissue plaque in the retroperitoneal space that often encases the aorta and one or both ureters resulting in obstruction. RPF is idiopathic in majority of the cases and has been associated with malignancy, autoimmune inflammatory disorders, GVHD, drugs, surgery, and multiple sclerosis in small number of cases. RPF usually affects males in their 4th–6th decades of life and often pre- sents with non-specific symptoms such as malaise, anorexia, and chronic backache. RPF is predominantly benign with a favorable prognosis. Small number cases, up to 8%, have been reported as malignant RPF with a poor prognosis and typical 3–6 months survival.”
Imaging of ureter: a primer for the emergency radiologist
Mohd Zahid et al.
Emergency Radiology (in press) - "The important distinguishing feature of benign RPF from malignant RPF, lymphoma, and metastatic lymph nodes is that the fibrotic plaque may extend behind the aorta and anterior to the spine but rarely displaces the aorta anteriorly, although it has poor sensitivity and specificity. Degree of enhancement of benign RPF on CT correlates with fibrotic activity, avid enhancement suggests active phase, and minimal to no enhancement seen in avascular chronic plaque. Variable enhancement pattern is also seen in malignant RPF. There is significant overlap between benign RPF and malignant RPF in imaging morphology and enhancement patterns.”
Imaging of ureter: a primer for the emergency radiologist
Mohd Zahid et al.
Emergency Radiology (in press) - "Malacoplakia is a rare granulomatous inflammatory disease of the genitourinary tract, but rarely may affect other organ systems. Most commonly, it occurs in the urinary bladder followed by the ureter and renal pelvis. Malacoplakia is caused by bacterial infection; Escherichia coli is the most common organism. Common presenting symptoms are flank pain, hematuria, and fever. On CT, common finding is segmental mural thickening of the ureter with or without proximal dilatation. Hydronephrosis is uncommon but can be seen and may result in renal dysfunction. Malacoplakia is usually diagnosed on biopsy and treated conservatively with antibiotics. It may require surgical plaque resection with possible ureteral stenting.”
Imaging of ureter: a primer for the emergency radiologist
Mohd Zahid et al.
Emergency Radiology (in press)
- “Over 80% of ectopic ureters are associated with duplicated systems and involve the upper moiety ureter. The ectopic ureteric insertion location often determines the clinical presentation. The ectopic ureteral orifice is always suprasphincteric, and the ureter inserts at the prostatic urethra, seminal vesicle, ejaculatory duct, or vas deferens in male patients.”
MDCT and MR Urogram Spectrum of Congenital Anomalies of the Kidney and Urinary Tract Diagnosed in Adulthood Surabhi VR et al. AJR 2015; 205:W294-W304 - “The ectopic ureteral orifice is always suprasphincteric, and the ureter inserts at the prostatic urethra, seminal vesicle, ejaculatory duct, or vas deferens in male patients.”
MDCT and MR Urogram Spectrum of Congenital Anomalies of the Kidney and Urinary Tract Diagnosed in Adulthood Surabhi VR et al. AJR 2015; 205:W294-W304 - “In female patients, the ectopic ureteral orifice may be either supra- or infrasphincteric, with the most common insertions being into the urethra or vaginal vestibule.”
MDCT and MR Urogram Spectrum of Congenital Anomalies of the Kidney and Urinary Tract Diagnosed in Adulthood Surabhi VR et al. AJR 2015; 205:W294-W304 - “The classic presentation of an ectopic ureter in female patients is continuous dribbling due to the insertion distal to the urethral sphincter. In male patients, the ectopic ureter inserts proximal to the sphincter, leading to nonspecific lower urinary tract symptoms, UTIs, and obstruction. CT or MR urogram provides great anatomic details and allows identification of ectopic insertion of ureter in both single and duplex collecting systems.”
MDCT and MR Urogram Spectrum of Congenital Anomalies of the Kidney and Urinary Tract Diagnosed in Adulthood Surabhi VR et al. AJR 2015; 205:W294-W304
- “Ectopic ureter is defined as abnormal insertion of the ureter, occurring in the posterior urethra in approximately 50% of cases in males. Other sites include the seminal vesicle (approximately one-third), vas deferens, bladder neck, prostate and epididymis, while the urethra and vagina are commonly affected in females.”
Ectopic insertion of the ureter into the seminal vesicle Mohamed Abou El-Ghar, Tarek El-Diasty World J Radiol. Sep 28, 2013; 5(9): 349-351 - “Ectopic insertion of the ureter is defined as abnormal insertion of the ureter, usually distal to the trigone into the urethra in male in approximately 50% of cases. Other sites include the seminal vesicle (approximately one-third), vas deferens, bladder neck, prostate and epididymis, while the urethra and vagina are commonly affected in females. Ectopic insertion of the ureter in the genital tract is a rare anomaly. Its incidence, as reported by Fraser, is about 1:130000. It is more common in females and is usually associated with incontinence, leading to the diagnosis, while in males, it is present with infection.”
Ectopic insertion of the ureter into the seminal vesicle Mohamed Abou El-Ghar, Tarek El-Diasty World J Radiol. Sep 28, 2013; 5(9): 349-351 - “Ectopic insertion of the ureter in the genital tract is a rare anomaly. Its incidence, as reported by Fraser, is about 1:130000. It is more common in females and is usually associated with incontinence, leading to the diagnosis, while in males, it is present with infection.”
Ectopic insertion of the ureter into the seminal vesicle Mohamed Abou El-Ghar, Tarek El-Diasty World J Radiol. Sep 28, 2013; 5(9): 349-351 - OBJECTIVE. The purpose of this study was to determine the value of clinical parameters and radiologic findings on unenhanced CT to the choice between interventional and conservative management for patients with acute renal colic.
CONCLUSION. Larger stone size, higher density, proximal location, and complaints of shivering, fever, and leukocytosis are the most important parameters for predicting invasive management of acute renal colic. Other clinical and radiologic information may be useful as supportive findings but do not predict the choice of patient management.
Can Unenhanced CT Findings Predict Interventional Versus Conservative Treatment in Acute Renal Colic? Lotan E et al. AJR 2016; 207:1016–1021
- "It remains retroperitoneal throughout its course, has an approximate length of 25 cm, and has a normal diameter of less than 3 mm. Histologically, it has an inner cell layer of watertight urothelium surrounded by an outer smooth muscle layer that allows coordinated contraction. Because of this ongoing peristalsis, excreted contrast agent may not be present throughout the ureter at CT urography if there is contraction within a given segment at the time of the examination."
CT Urography for Evaluation of the Ureter
Potenta SE et al
RadioGraphics 2015; 35:709-726 - "The Weigert-Meyer rule states that in a complete duplication, the upper pole ureter terminates inferior and medial to the lower pole ureter."
CT Urography for Evaluation of the Ureter
Potenta SE et al
RadioGraphics 2015; 35:709-726 - "UCC occurs most commonly in elderly men. The risk factors include smoking, occupational exposure to chemical carcinogens (eg, in the textile and plastics industries), and a history of cyclophosphamide or phenacetin use. Because of field effect from these exposures, the entire urinary tract is susceptible to malignant transformation. As a result, UCC is often multi- focal at presentation, and the entire urinary tract should be scrutinized for synchronous lesions if a single lesion is found."
CT Urography for Evaluation of the Ureter
Potenta SE et al
RadioGraphics 2015; 35:709-726 - "Other tumors that can cause ureteral filling defects include squamous cell carcinoma (SCC) and metastases. SCC is much less common than UCC in Western countries but has an increased incidence in countries where schistosomiasis is endemic. SCC and UCC cannot be reliably distinguished at CT urography."
CT Urography for Evaluation of the Ureter
Potenta SE et al
RadioGraphics 2015; 35:709-726 - "Inflammatory and hyperplastic lesions of the ureter are uncommon and can manifest as soli- tary or multiple filling defects.These benign lesions cannot be reliably distinguished from tumors at CT urography, and uretero- scopic evaluation is often necessary. Multiple filling defects can be due to benign entities such as polyureteritis cystica or malacoplakia; however, multifocal UCC can have a similar appearance. Polyureteritis cystica manifests as multiple small (a few millimeters) round filling defects, often in a proximal distribution, which tend to be more numerous than those in multi- focal UCC."
CT Urography for Evaluation of the Ureter
Potenta SE et al
RadioGraphics 2015; 35:709-726 - "Ureteral thickening with associated enhancement and periureteral stranding is often found in the setting of infectious ureteritis. Ureteritis can be seen in the setting of cystitis, pyelonephritis, or pyonephrosis. Although discrete filling defects are uncommonly caused by infection, a few infections, such as tuberculosis, fungus, and schistosomes, occasionally produce this imaging finding."
CT Urography for Evaluation of the Ureter
Potenta SE et al
RadioGraphics 2015; 35:709-726 - "Renal papillary necrosis is the predominant cause of an ischemic filling defect, and its etiology includes analgesic abuse or overuse, sickle cell disease, pyelonephritis, renal vein thrombosis, tuberculosis, obstructive uropathy, and diabetes. Necrotic papillae can become dislodged and fall into the ureter, potentially resulting in hydronephrosis. If a ureteral filling defect is identified at CT urography, it is important to look for signs of papillary necrosis as a potential cause. Associated findings include caliceal cavities and blunting. "
CT Urography for Evaluation of the Ureter
Potenta SE et al
RadioGraphics 2015; 35:709-726 - Dilated Ureter: Unilateral
● Obstructed ureter from any of the following causes:
● Calculus
● Tumor
● Clot
● Sloughed papilla from papillary necrosis
● Stricture
● Extrinsic compression
● Mass effect
● Residual dilatation from a previously resolved obstruction (particularly if the distention was severe) - Dilated Ureter: Bilateral
● Obstructed ureters from any of the following causes:
● Polyuria or diuresis (eg, medication, diabetes insipidus)
● Bladder outlet obstruction
● Neurogenic bladder
● Pregnancy (more pronounced on right side) - Dilated Ureter: Congenital
● Obstructed unilateral or bilateral
● Vesicoureteral reflux
● Primary megaureter (≥7-mm dilatation)
● Ectopic ureter
● Ureterocele
● Prune belly syndrome (bilateral)
- “The ureter is a muscular conduit that carries urine from the renal pelvis to the urinary bladder. It arises proximally from the renal pelvis at the ureteropelvic junction (UPJ) and empties distally into the urinary bladder at the ureterovesicular junction (UVJ). It remains retroperitoneal throughout its course, has an approximate length of 25 cm, and has a normal diameter of less than 3 mm. Histologically, it has an inner cell layer of watertight urothelium surrounded by an outer smooth muscle layer that allows coordinated contraction. Because of this ongoing peristalsis, excreted contrast agent may not be present throughout the ureter at CT urography if there is contraction within a given segment at the time of the examination.”
CT Urography for Evaluation of the Ureter Potenta SE et al. Radiographics. 2015 May-Jun;35(3):709-26 - “A dilated ureter is not necessarily obstructed; conversely, an obstructed ureter is not always dilated.”
CT Urography for Evaluation of the Ureter Potenta SE et al. Radiographics. 2015 May-Jun;35(3):709-26 - “Any ureteral filling defect that demonstrates soft-tissue attenu- ation should be considered malignant until proven otherwise and generally requires ureteroscopic evaluation, biopsy, and cytologic analysis.”
CT Urography for Evaluation of the Ureter Potenta SE et al. Radiographics. 2015 May-Jun;35(3):709-26 - “Any ureteral filling defect that demonstrates soft-tissue attenuation should be considered malignant until proven otherwise and generally requires ureteroscopic evaluation, biopsy, and cytologic analysis.
A dilated ureter is not necessarily obstructed; conversely, an obstructed ureter is not always dilated.
Physiologic narrowing is common and is most easily identified by absence of proximal dilatation and by changeability in different acquisitions. A stricture is defined as a fixed narrowing with proximal dilatation.”
CT Urography for Evaluation of the Ureter Potenta SE et al. Radiographics. 2015 May-Jun;35(3):709-26 - “The ureter is a muscular conduit that carries urine from the renal pelvis to the urinary bladder. It arises proximally from the renal pelvis at the ureteropelvic junction (UPJ) and empties distally into the urinary bladder at the ureterovesicular junction (UVJ) . It remains retroperitoneal throughout its course, has an approximate length of 25 cm, and has a normal diameter of less than 3 mm.”
CT Urography for Evaluation of the Ureter Potenta SE et al. Radiographics. 2015 May-Jun;35(3):709-26 - “Ureteral duplication is the most common congenital anomaly of the urinary tract and occurs in approximately 1% of the population. Duplications can occur unilaterally or bilaterally and can be partial or complete.”
CT Urography for Evaluation of the Ureter Potenta SE et al. Radiographics. 2015 May-Jun;35(3):709-26 - “UPJ obstruction is the most common cause of prenatal hydronephrosis, although it may go undiagnosed until later in life. In particular, Dietl’s crisis (also known as “beer-drinker’s hydronephrosis”) refers to a UPJ obstruction that manifests as intermittent flank pain that typically occurs after a large volume of fluid intake and subsequent diuresis (classically seen in college freshmen after excessive alcohol intake).These patients become symptomatic when the rate of excretion exceeds the flow rate through the narrowed UPJ.”
CT Urography for Evaluation of the Ureter Potenta SE et al. Radiographics. 2015 May-Jun;35(3):709-26 - “A ureteral clot can form after an intraureteral hemorrhage due to trauma, calculi, underlying malignancy, or anticoagulation. At imaging, clot material can appear as a small rounded filling defect or as a vermiform defect that fills the ureter. A clot does not enhance and can be identified on a nonenhanced image as hyperattenuating (>50 HU) relative both to urine and the surrounding soft tissues, occasionally with a urine-clot interface. A clot also resolves at follow-up imaging studies. However, a small clot may be difficult to distinguish from UCC at ini- tial identification at CT urography, and ureteros- copy and/or short-interval follow-up imaging may be necessary.”
CT Urography for Evaluation of the Ureter Potenta SE et al. Radiographics. 2015 May-Jun;35(3):709-26 - “Ureteral thickening with associated enhancement and periureteral stranding is often found in the setting of infectious ureteritis. Ureteritis can be seen in the setting of cystitis, pyelonephritis, or pyonephrosis. Although discrete filling defects are uncommonly caused by infection, a few infections, such as tuberculosis, fungus, and schistosomes, occasionally produce this imaging finding.”
CT Urography for Evaluation of the Ureter Potenta SE et al. Radiographics. 2015 May-Jun;35(3):709-26 - “Renal papillary necrosis is the predominant cause of an ischemic filling defect, and its etiol-
ogy includes analgesic abuse or overuse, sickle cell disease, pyelonephritis, renal vein thrombosis, tuberculosis, obstructive uropathy, and diabetes. Necrotic papillae can become dislodged and fall into the ureter, potentially resulting in hydronephrosis. If a ureteral filling defect is identified at CT urography, it is important to look for signs of papillary necrosis as a potential cause. Associated findings include caliceal cavities and blunting.”
CT Urography for Evaluation of the Ureter Potenta SE et al. Radiographics. 2015 May-Jun;35(3):709-26 - Causes of Deviated Ureter: Differential Diagnosis
- Surgical diversion: Ileal conduit Continent cutaneous diversion Orthotopic neobladder
- Trauma
- Local mass effect (eg, lymphoma, pelvic mass, aneurysm)
- Ureteral fistula
- Congenital retrocaval or circumcaval ureter
- Retroperitoneal fibrosis (medial deviation)
- Inflammatory aortic aneurysm (medial deviation)
- Herniated ureter through inguinal canal (rare)
- CTA Evaluation of Suspected UPJ Obstruction
- In the context of UPJO, “crossing vessels” are those renal arteries or veins found in the region of the ureteric transition point. The normal renal arteries may be single or multiple and give rise to anterior and posterior branches. The right renal artery normally crosses posterior to the vena cava. Arteries crossing anterior to the vena cava have been implicated in UPJO
- Most crossing vessels are renal arteries and are anterior. The anterior vessel branches supply the superior and middle renal segments with a lower-segment branch to the anterior and posterior lower pole. The posterior branch arches over the renal pelvis to supply the smaller corresponding superior and middle posterior segments. All renal arteries are end arteries and thus should be sacrificed for UPJO treatment only after thorough consideration of their role in the process of obstruction. The lower-pole segmental artery or vein in particular has been implicated in UPJO. When crossing vessels are observed, it is tempting to implicate them in the etiology of UPJO, although in many cases they may be “innocent bystanders.”
- The distended renal pelvis secondary to UPJO is largely extrarenal and of necessity will balloon over a lower renal segmental vessel when a potential space is created between it and the adjacent main renal artery.
- “ Even when well distended, ureteral tumors can be extremely subtle and difficult to detect, particularly when relying primarily on the source axial images.”
MDCT Evaluation of Ureteral Tumors: Advantages of 3D Reconstruction and Volume Visualization
Raman SP, Horton KM, Fishman EK
AJR 2013; 201;1239-1247 - “ The ureters can be problematic to evaluate on CT, partly because of difficulties in obtaining adequate ureteral distention and opacification. Proper diagnosis hinges not only on appropriate interpretation of the axial images but also on the utilization of a 3D technique (volume rendering or maximum intensity projection) as an ancillary tool.”
MDCT Evaluation of Ureteral Tumors: Advantages of 3D Reconstruction and Volume Visualization
Raman SP, Horton KM, Fishman EK
AJR 2013; 201;1239-1247 - “ We have seen numerous TCCs initially missed on a review of the axial images and multiplanar reformations but subsequently diagnosed on the 3D images.”
MDCT Evaluation of Ureteral Tumors: Advantages of 3D Reconstruction and Volume Visualization
Raman SP, Horton KM, Fishman EK
AJR 2013; 201;1239-1247 - “ In our experience, proper utilization of a 3D technique can be incredibly useful in the diagnosis of subtle tumors that are barely perceptible on the source axial images and that may be missed otherwise.”
MDCT Evaluation of Ureteral Tumors: Advantages of 3D Reconstruction and Volume Visualization
Raman SP, Horton KM, Fishman EK
AJR 2013; 201;1239-1247 - Advantages of 3D Imaging
- Accentuation of subtle strictures and site of narrowing
- Abnormal urothelial enhancement and thickening accentuated
- Evaluation of distal ureters optimized
- Flat polypoid lesions easier to visualize - Ureteral Tumors: Facts
- Lesions are most common in the distal ureter (73%) compared with mid (24%) and proximal (3%) ureter
- Transitional cell carcinoma accounts for 90% of ureteral tumors with squamous cell carcinoma (10%) and adenocarcinoma (1%) uncommon
- Average age over age 60 and more common in men than woman
- Risk factors include analgesic overuse (including phenacetin) and chemical carcinogens (aniline dyes) - Ureteral Tumors: Differential Dx
- Transitional cell carcinoma (TCC)
- Squamous cell carcinoma
- Adenocarcinoma
- Lymphoma
- Metastases (breast cancer, GI tract malignancies, prostate cancer, cervical cancer, and renal cell carcinoma - CT of the Ureter: CT Findings
- Urothelial thickening is most common finding
- Urothelial enhancement
- Ureteral calcification
- Periureteral fat stranding
- Filling defect or mass
- Hydronephrosis and hydroureter
- Ureteral TCC:
Imaging Findings
- Urothelial thickening
- Abnormal urothelial enhancement
- Particularly when asymmetric, focal, and in conjunction with thickening
- Ureteral calcification
- Periureteral fat stranding
- Discrete filling defect or mass
- Look for site of transition and proximal hydronephrosis & hydroureter
- How large is a normal Ureter on CT-
“The mean size of ureters on the asymptomatic side was 1.8 mm with a standard deviation (SD) of 0.9 mm. The mean size of ureters on the obstructed side was 7 mm with an SD of 3.2 mm. In 96% of patients, the ureter diameter on the asymptomatic side was 3 mm or smaller.”
Normal Ureter Size on Unenhanced Helical C
TZelenko N et al.
AJR 2004; 182:1039-1041 - “The mean size of ureters on the asymptomatic side was 1.8 mm with a standard deviation (SD) of 0.9 mm. The mean size of ureters on the obstructed side was 7 mm with an SD of 3.2 mm. In 96% of patients, the ureter diameter on the asymptomatic side was 3 mm or smaller.”
Normal Ureter Size on on Unenhanced Helical CT
Zelenko n et al.
AJR 2004;182:1039–1041 - “In view of the fact that correctly identifying ureteral dilatation may be crucial to arrive at a correct diagnosis, the need for a definition of what constitutes ureteral dilatation on unenhanced CT is clear. On the basis of the results of this study, we have established 3 mm as the upper limit of normal for ureter diameter on unenhanced CT. Although for many cases reliance on such a measurement will be unnecessary, in the more complex cases and for more inexperienced observers, such a measurement may be helpful.”
Normal Ureter Size on on Unenhanced Helical CT
Zelenko n et al.
AJR 2004;182:1039–1041 - “However, evaluation of the ureters using CT can be particularly problematic. Not only are the ureters often poorly opacified and distended due to poor CT technique, but the majority of ureteral TCC’s are found in the distal third of the ureters, a segment that is particularly difficult to completely distend. Moreover, even when well distended, ureteral tumors can be extremely subtle and difficult to appreciate, particularly when relying primarily on the source axial images.”
MDCT Evaluation of Ureteral Tumors:
Advantages of 3-D Reconstruction and Volume Visualization
Raman SP, Horton KM, Fishman EK
AJR (in press) - “While ureteral TCC’s can occur in any portion of the ureter, the most common location is thought to be the renal pelvis, accounting for 15% of all renal tumors, likely as a result of the large area of urothelium in this location. Within the ureter itself, TCC’s of the distal ureter are much more common (73%) compared to lesions in the mid (24%) and proximal ureters (3%).”
MDCT Evaluation of Ureteral Tumors:
Advantages of 3-D Reconstruction and Volume Visualization
Raman SP, Horton KM, Fishman EK
AJR (in press) - “While the ureters must be looked upon with suspicion in any patient who presents for a CT examination with either gross or microscopic hematuria, the pretest probability increases markedly in patients with a known bladder TCC: 2-4% of patients with bladder TCC’s ultimately develop an upper tract TCC, making it vital that this subgroup of patients undergoes CT urography not only at initial presentation, but also during routine follow-up.”
MDCT Evaluation of Ureteral Tumors:
Advantages of 3-D Reconstruction and Volume Visualization
Raman SP, Horton KM, Fishman EK
AJR (in press) - “Most TCC’s occur in patients over the age of 60, and men are at greater risk compared to women. Major risk factors include increasing age, male gender, smoking, analgesic overuse (including phenacetin), and a variety of chemical carcinogens (most notably aniline dyes). It is believed that the majority of the carcinogens that predispose towards TCC are excreted into the urine, where they directly interact with the adjacent urothelium.”
MDCT Evaluation of Ureteral Tumors:
Advantages of 3-D Reconstruction and Volume Visualization
Raman SP, Horton KM, Fishman EK
AJR (in press) - TCC of the Kidney and Ureter: Facts
- Age over age 60 (increases with age)
- Men at greater risk than woman (M>F)
- Other risk factors include;
- Smoking
- Analgesic overuse (phenactin)
- Chemical carcinogens (aniline dyes)
- “Balkan Nephropathy” (200x risk of TCC) - Ureteral Tumors: Differential Diagnosis
- Transitional cell carcinoma
- Lymphoma
- Metastases
- Breast cancer
- GI tract malignancies
- Prostate cancer
- Cervical cancer
- Renal cell carcinoma - CT Techniques for Evaluating the Ureter
- Contrast Injection Protocols
- Single bolus technique
- Split bolus technique
- Triple bolus technique
- Protocol Options
- Compression techniques
- IV saline
- IV furosemide
- Prone positioning - JHH CT Technique for Evaluating the Ureter
- 1000 cc of water over a 15-20 minute period prior to the study
- 100-120 cc of Omnipaque-350 injected 4-5 cc/sec
- Delayed phase images acquired at 5 minutes post injection unless study is done for UPJ obstruction and then delay is 8-10 minutes - CT of the Ureter: Data Analysis
- Axial images reviewed at .75mm-3mm
- Coronal and Sagittal or Oblique MPRs
- Volume Rendering and MIP Images - CT of the Ureter: Imaging Features of Malignancy
- Urothelial Thickening
- Urothelial Enhancement
- Ureteral Calcifications
- Periureteral fat stranding
- Filling defect/mass
- Hydronephrosis and Hydroureter (transition points) - CT of the Ureter: Role of 3D Imaging in Lesion Detection
- Accentuation of subtle strictures and sites of narrowing
- Accentuate subtle abnormal urothelial enhancement and thickening
- Better visualization of the distal ureter
- Better visualization of flat polypoid lesions - “Most TCC’s occur in patients over the age of 60, and men are at greater risk compared to women. Major risk factors include increasing age, male gender, smoking, analgesic overuse (including phenacetin), and a variety of chemical carcinogens (most notably aniline dyes). It is believed that the majority of the carcinogens that predispose towards TCC are excreted into the urine, where they directly interact with the adjacent urothelium.”
MDCT Evaluation of Ureteral Tumors:
Advantages of 3-D Reconstruction and Volume Visualization
Raman SP, Horton KM, Fishman EK
AJR (in press) - “Proper diagnosis hinges not only on appropriate interpretation of the source axial images (with recognition of several suggestive CT features of malignancy), but also upon the utilization of 3-D technique (CR and MIP technique) as an ancillary diagnostic tool. In our experience, proper utilization of 3-D technique can be incredibly useful in the diagnosis of subtle tumors that are barely perceptible on the source axial images, and which may be missed otherwise.”
MDCT Evaluation of Ureteral Tumors:
Advantages of 3-D Reconstruction and Volume Visualization
Raman SP, Horton KM, Fishman EK
AJR (in press)
- Purpose: “ To determine whether ureteral segments not filled with contrast material at computed tomographic (CT) urography ever contain tumor detectable only by filling these segments with contrast material”
Conclusion: “ Targeted delayed scanning at CT urography yielded no additional ureteral tumors and resulted in additional radiation exposure.”
Targeted Delayed Scanning at CT Urography: A Worthwhile Use of Radiation?
Hack K et al.
Radiology 2012; 265:143-150 - “ In patients undergoing CT urography for detection of neoplasms, routine additional excretory phase imaging to attempt complete ureteral opacification is not advised, given the low likelihood that the sole manifestation of a tumor will be a filling defect in an otherwise normal ureter.”
Targeted Delayed Scanning at CT Urography: A Worthwhile Use of Radiation?
Hack K et al.
Radiology 2012; 265:143-150 - “ Given the added radiation associated with performing additional delayed scanning, we recommend obtaining only a single additional delayed scan for ureteral nonopacification.”
Targeted Delayed Scanning at CT Urography: A Worthwhile Use of Radiation?
Hack K et al.
Radiology 2012; 265:143-150