|
-- OR -- |
|
- “The 3D endoluminal fly-through provides a highly effective detection mechanism for focal colorectal lesions . The lack of easy, automated centerline navigation has been a major drawback with most other CTC systems, but continued improvement has been shown by some. UWHC’s primary 3D review for the DoD trial initially entailed bidirectional fly-through using a 90° field-of-view (FOV) angle on both supine and prone series. However, they have since found that widening the FOV angle to 120° allows greatly improved mucosal visualization, generally allowing for one-way fly-through of each series (rectum-to-cecum on supine and cecum-to-rectum on prone) without sacrificing polyp detection.
Bidirectional fly-through at 120°on at least one series remains prudent, however, for cases with suboptimal distention.” Imaging and Screening for Colorectal Cancer with CT Colonography. Pickhardt PJ Radiol Clin North Am. 2017 Nov;55(6):1183-1196 - “When a suspicious lesion measuring 5 to 6 mm or greater is detected on 3D (or 2D) and confirmed to be composed of soft tissue on 2D, an electronic bookmark is placed on the colon map. The vast majority of actual polyps can also be identified on the alternate supine or prone view, which greatly increases overall diagnostic confidence. Those at UWHC have found computer-aided detection (CAD) to be useful in both the research and clinical settings, because it can provide further assurance and diagnostic confidence . CAD demonstrates excellent sensitivity for detecting relevant polyps, but the extremely low specificity, which essentially approached zero, requires that experienced CTC readers sift through the CAD marks, not novice readers.”
Imaging and Screening for Colorectal Cancer with CT Colonography. Pickhardt PJ Radiol Clin North Am. 2017 Nov;55(6):1183-1196 - “Approximately 85% to 90% of screening CTC 2examinations are negative for polyps ≥6 mm, and repeat routine colorectal screening is recommended in 5 years. Nonreporting of potential isolated diminutive lesions is justified to prevent unnecessary interventions, and this practice has been clinically validated. This practice is explicitly described in the dictation template. For individuals who are found to be negative at follow-up screening CTC at 5 or more years, subsequent screening can likely be extended out to 10 years.”
Imaging and Screening for Colorectal Cancer with CT Colonography. Pickhardt PJ Radiol Clin North Am. 2017 Nov;55(6):1183-1196 - “Despite being readily preventable, CRC remains the second-leading cause of cancer deaths. If preventive screening tests that effectively detect advanced adenomas and early cancers were broadly applied, this situation could be easily reversed. CT colonography reflects an ideal balance of minimal invasiveness with high-level performance, assuming all facets of the examination are appropriately addressed. Nonetheless, this promising screening test remains grossly underused. This review of the technical and interpretive approaches used by one successful CTC screening program may serve as a roadmap to other groups looking to get involved.”
Imaging and Screening for Colorectal Cancer with CT Colonography. Pickhardt PJ Radiol Clin North Am. 2017 Nov;55(6):1183-1196
- Challenges for Virtual Colonoscopy
• Extra-colonic findings
• Potential of missing small expecially flat lesions
• Physican training for interpretation of the studies
• Physician acceptance of the procedure
• Cost of equipment
• Reimbursement - “Of the 11.7% (927/7952) of patients in our cohort with indeterminate or potentially significant extracolonic findings, 9.1% (725/7952) of findings were classified as E3 and 2.5% of findings (202/7952) were classified as E4; these figures are also consistent with prior studies .Because E4 findings are of the highest clinical suspicion, nearly all of these receive further workup or attention; further workup of E3 findings is substantialy more heterogeneous and is often subject to referring provider and patient preference.”
Extracolonic Findings at Screening CT Colonography: Prevalence, Benefits, Challenges, and Opportunities B. Dustin Pooler, David H. Kim, Perry J. Pickhardt AJR 2017; 209:1–9 - “Another key benefit of extracolonic evaluation at CTC that is often overlooked is the simple reassurance provided to the majority of patients (nearly 90%) for whom nothing of concern is found in the abdomen or pelvis. This negative information provides peace of mind that is rarely measured in research, but is nonetheless highly valued by patients.”
Extracolonic Findings at Screening CT Colonography: Prevalence, Benefits, Challenges, and Opportunities B. Dustin Pooler, David H. Kim, Perry J. Pickhardt AJR 2017; 209:1–9 - “Yet another potential bene t of extracolonic evaluation at CTC is the ability to provide opportunistic or synergistic screening for other conditions, most notably osteoporosis, as well as AAA and extracolonic cancer screening .”
Extracolonic Findings at Screening CT Colonography: Prevalence, Benefits, Challenges, and Opportunities B. Dustin Pooler, David H. Kim, Perry J. Pickhardt AJR 2017; 209:1–9 - “Although concern persists in some circles regarding the issue of extracolonic ndings at screening CTC, there is little in the literature to suggest that it causes substantial harm or has excessive cost, and a growing body of lit- erature suggests that there is additional value added in the form of detection of clinically significant disease and opportunities for additional screening outside the colon.”
Extracolonic Findings at Screening CT Colonography: Prevalence, Benefits, Challenges, and Opportunities B. Dustin Pooler, David H. Kim, Perry J. Pickhardt AJR 2017; 209:1–9 - “For those patients with E3 and E4 findings, a substantial percentage (20% overall and nearly 70% of E4 patients in our experience) will ultimately receive a diagnosis of previously unsuspected clinically relevant disease, typically requiring either treatment or surveillance. Most of the remaining cases will have benign conditions confirmed with either follow-up imaging or clinical follow-up alone, and less than 0.5% of all patients undergoing screening CTC will undergo invasive biopsy or surgery to prove a benign condition.”
Extracolonic Findings at Screening CT Colonography: Prevalence, Benefits, Challenges, and Opportunities B. Dustin Pooler, David H. Kim, Perry J. Pickhardt AJR 2017; 209:1–9 - Virtual Colonoscopy Bowel Prep
• Diet
• Catharsis
- PEG (polyethylene glycol)
- Glycolax
- Magnesium citrate
• Tagging
- Barium
- Omnipaue-350 (50 cc before bedtime) - Johns Hopkins Prep Schedule
8AM
Clear liquid breakfast with 1 bottle barium.
Mix 4L PEG and put in Frig
Noon
Clear liquid lunch with 1/2 bottle of barium in 4 oz water
3PM
Drink 8 oz PEG every 15 minutes until gone (4-5 hours)
5PM
Drink 1/2 bottle barium in 4 oz
8PM
Take 2 bisacodyl tablets
Bedtime
50cc Iohexol mixed in 8oz sprite - Colon Distension with CO2
Electronic CO2 insufflator
- Image Interpretation: 2D vs 3D



- “Optical colonoscopy complications that can be detected at CT include bowel perforation, postprocedural hemorrhage, postpolypectomy syndrome, splenic injury, appendicitis, and diverticulitis. Radiologist awareness of optical colonoscopy complications seen at CT is imperative for appropriate diagnosis and prompt patient management.”
Acute Abdominal Pain Following Optical Colonoscopy: CT Findings and Clinical Considerations Levenson RB et al. AJR 2016; 207:W33–W40 - “Although serious optical colonoscopy complications are uncommon, reportedly in 0.1–0.3% of cases overall and in up to 5% of cases after biopsy, polypectomy, or other therapeutic procedure, they can be life-threatening if not quickly recognized. Interventions performed during optical colonoscopy increase the chance of complication; over 85% of complications are reported in patients undergoing optical colonoscopy with polypectomy.”
Acute Abdominal Pain Following Optical Colonoscopy: CT Findings and Clinical Considerations Levenson RB et al. AJR 2016; 207:W33–W40 - “Bowel perforation may occur relatively rarely from optical colonoscopy, occurring in ≤ 0.3% of screening colonoscopies up to 0.03–0.8% for diagnostic colonoscopy and 0.15–3% for therapeutic colonoscopy .”
Acute Abdominal Pain Following Optical Colonoscopy: CT Findings and Clinical Considerations Levenson RB et al. AJR 2016; 207:W33–W40 - “Intraluminal hemorrhage is the most com- mon major complication after optical colonos- copy. Although most patients do not undergo CT, their diagnosis and management is man- aged by the gastroenterologist (and other clinicians). Postcolonoscopy hemorrhage has been reported to occur in 1–6 of every 1000 colonoscopies. The rate is greater in patients who have undergone polypectomy (2.1– 3.7 per 1000 examinations, compared with 8.7 per 1000 examinations).”
Acute Abdominal Pain Following Optical Colonoscopy: CT Findings and Clinical Considerations Levenson RB et al. AJR 2016; 207:W33–W40 - “Electrocoagulation injury to the bowel wall from electrical current applied during polypectomy induces a transmural burn and localized peritonitis without evidence of perforation on imaging examinations. Patients typically present within 12 hours with abdominal pain and tenderness, but symptoms may present up to 5 days after the procedure . Patients may also have fever, leukocytosis, and tachycardia, which can clinically mimic bowel perforation.”
Acute Abdominal Pain Following Optical Colonoscopy: CT Findings and Clinical Considerations Levenson RB et al. AJR 2016; 207:W33–W40 - “Postcolonoscopy complications that may be seen in patients in the ED include bowel perforation, postprocedural hemorrhage, postpolypectomy syndrome, splenic injury, appendicitis, and diverticulitis. CT is the imaging modality of choice in the ED, allowing rapid detection of these various complications. Although postcolonoscopy complica- tions are infrequent, radiologist awareness of these complications and the associated imaging findings is essential for optimal diagnosis and prompt management.”
Acute Abdominal Pain Following Optical Colonoscopy: CT Findings and Clinical Considerations Levenson RB et al. AJR 2016; 207:W33–W40
- “In a prospective study, first degree relatives at least 40 years old, identified from consecutive patients admitted with colorectal cancer, underwent noncathartic CT colonography and colonoscopy the day after; the sensitivity and specificity of CT colonography for polyps measuring at least 6 were 77% and 99% respectively.”
Noncathartic CT Colonography to Screen for Colorectal Neoplasia in Subjects with a Family History of Colorectal Cancer
Fini L et al.
Radiology 2014; 270:784-790 - “ Noncathartic CT colonography could be offered as a noninvasive alternative to colonoscopy in prevention programs for first degree relatives of patients with colorectal cancer.”
Noncathartic CT Colonography to Screen for Colorectal Neoplasia in Subjects with a Family History of Colorectal Cancer
Fini L et al.
Radiology 2014; 270:784-790
- NY Times article recommendations
“ Respondents reported a very high satisfaction level with CTC, and those who had experienced both modalities indicated a preference for CTC over optical colonoscopy. These results suggest that CTC has the potential to increase adherence to CRC screening guidelines if widely available.”
Screening CT Colonography: Multicenter Survey of Patient Experience, Preference and Potential Impact on Adherence
Pooler BD et al.
AJR 2012; 198:1361-1366 - “ Of 441 patients who had experienced both CTC and optical colonoscopy, 77.1% preferred CTC and 13.8% preferred optical colonoscopy. Of all patients 29.6% indicated that they may not have undergone optical colonoscopy screening if CTC were not available.”
Screening CT Colonography: Multicenter Survey of Patient Experience, Preference and Potential Impact on Adherence
Pooler BD et al.
AJR 2012; 198:1361-1366
- “ For most measures of diagnostic performance and in most subsets, the difference between senior-aged participants and those younger than 65 years was not statistically different.”
The National CT Colonography Trial: Assessment of Accuracy in Participants 65 Years of Age and Older
Johnson CD et a.
Radiology 2012; 263:401-408 - “ There was no significant difference in the accuracy of CT colonography for the detection of large and intermediate sized adenomatous lesions in participants aged 65 years or older compared with that of younger participants; per participant sensitivity and specificity among the older and younger cohorts were 0.82 and 0.83 and 0.92 and 0.86 respectively.”
The National CT Colonography Trial: Assessment of Accuracy in Participants 65 Years of Age and Older
Johnson CD et a.
Radiology 2012; 263:401-408 - “ CT colonography can be used as a primary colorectal screening tool in patients older than 65 years, as well as in those aged 50-65 years.”
The National CT Colonography Trial: Assessment of Accuracy in Participants 65 Years of Age and Older
Johnson CD et a.
Radiology 2012; 263:401-408
- “Forty nine studies provided data on 11,151 patients with a cumulative colorectal cancer prevalence of 3.6% (414 cancers). The sensitivity of CT colonography for colorectal cancer was 96.1% (398 of 414;95% confidence interval:93.8%,97.7%). No heterogeneity was detected. No cancers were missed at CT colonography when both cathartic and tagging agents were combined in the bowel preparation. The sensitivity ofOC for colorectal cancer derived from a subset of 25 studies including 9223 patients, was 94.7% (178 of 188).”
Colorectal Cancer: CT Colonography and Colonoscopy for Detection-Systematic Review and Meta-Analysis
Pickhardt PJ et al
Radiology 2011; 259:393-405 - “CT colonography is highly sensitive for colorectal cancer detection across a broad spectrum of accepted indications, protocols, and techniques, with an overall sensitivity in published trials of 96.1%.”
Colorectal Cancer: CT Colonography and Colonoscopy for Detection-Systematic Review and Meta-Analysis
Pickhardt PJ et al
Radiology 2011; 259:393-405 - “ CT colonography is highly sensitive for colorectal cancer, especially when both cathartic and tagging agents are combined in the bowel preparation. Given the relatively low prevalence of colorectal cancer, primary CT colonography may be more suitable than OC (optical colonoscopy) for initial investigation of suspected colorectal cancer, assuming reasonable specificity.”
Colorectal Cancer: CT Colonography and Colonoscopy for Detection-Systematic Review and meta-Analysis
Pickhardt PJ et al
Radiology 2011; 259:393-405 - “ For CT colonographic examinations with polyps 6 mm or larger and 10 mm or larger, sensitivity and specificity, respectively were not significantly different when readers with a preference for primary 2D (0.84 and 0.86), a preference for primary 3D (0.76 and 0.82), or a preference for both 2D and 3D (0.84 and 0.83) were compared.”
ACRIN CT Colonography Trial: Does Reader’s Preference for Primary Two-Dimensional versus Primary Three-Dimensional Interpretation Affect Performance?
Hara AK et al.
Radiology 2011;259:435-441 - “ The reader’s preference for interpretive method had no effect on CT colonographic performance.”
ACRIN CT Colonography Trial: Does Reader’s Preference for Primary Two-Dimensional versus Primary Three-Dimensional Interpretation Affect Performance?
Hara AK et al.
Radiology 2011;259:435-441 "CTC increased the odds of identifying high risk lesions by 78%. CTC should be considered as an alternative to optical colonoscopy for colorectal cancer screening or as a onetime procedure to identify significant treatable intracolonic and extracolonic lesions"
Extracolonic Findings on CT Colonography Increases Yield of Colorectal Cancer Screening
Veerappan GR et al
AJR 2010; 195:677-686- Other identified reasons for CTC Selection
- Personal recommendation
- Ability to detect extracolonic pathology
- Poor previous colonoscopy experience
- Incomplete colonoscopy in the past "Two hundred fifty consecutive average-risk patients undergoing CRC screening completed a survey that assessed reasons for choosing CTC in lieu of colonoscopy, compliance with CRC screening if CTC was not offerred, and which of the two tests they preferred."
CT Colonography May Improve Colorectal Cancer Screening Compliance
Moawad FJ et al
AJR 2010; 195:1118-1123"Among the 57 patients who had experienced both procedures, 95% (n=54) preferred CTC."
CT Colonography May Improve Colorectal Cancer Screening Compliance
Moawad FJ et al
AJR 2010; 195:1118-1123"The most common reasons for undergoing CTC included convenience (33.6%), recommenation by referring provider (13.2%), and percieved safety (10.8%). Had CTC not been an available option, 91 of 250 patients (36%) would have foregone CRC screening."
CT Colonography May Improve Colorectal Cancer Screening Compliance
Moawad FJ et al
AJR 2010; 195:1118-1123- Colorectal Cancer: Risk Categories
- 1. average risk (age of 50 years old)
- 2. moderate risk (first degree relative with a history of adenoma or carcinoma or personal history of adenoma or carcinoma)
- 3. high risk (hereditary syndromes like familial polyposis, personal history of ulcerative colitis or Crohn’s disease) - Why do we do Colon Cancer screening?
- The prevalence of adenomas in the general population is 30-50% and increases with age
- The vast majority of adenomas are <1cm and these lesions have about a 1% likelihood of containing invasive cancer.
- Only 1-3% of adenomas ever progress to cancer
- Adenomas >1 cm have have a 10% chance of containing invasive cancer and a 25% chance of progressing to invasive cancer over 20 years
- Approximately 8% may undergo malignant degeneration within 10 years - ACR Appropriateness Criteria on Colorectal Cancer Screening: Summary Statements
- Computed tomographic colonography has emerged as the leading imaging technique for colorectal cancer screening
- The DCBE remains an imaging test that is also appropriate for colorectal cancer screening, particularly when CTC is not available
- Computed tomographic colonography is the preferred test after incomplete colonoscopy
- Imaging tests, including CTC and barium enema, are usually not appropriate for colorectal cancer screening in high risk patients with hereditary nonpolyposis colrectal cancer and inflammatory bowel disease "In 2008, the American Cancer Society guideline for colorectal cancer screening was revised jointly with the US Multi-Society Task Force on Colorectal Cancer and the ACR to include CTC every 5 years as an option for average risk patients."
ACR Appropriateness Criteria on Colorectal Cancer Screening
Yee J et al.
J Am Coll Radiol 2010;7:670-678"Seven high risk lesions were identified(six extracolonic malignancies and one large aortic aneurysm) in patients with significant findings. CTC also identified six intracolonic malignancies and three adenomas with high grade dysplasias. When considering extracolonic findings, CTC increased the odds of identifying high risk lesions by 78% (9 vs 16)."
Extracolonic Findings on CT Colonography Increases Yield of Colorectal Cancer Screening
Veerappan GR et al
AJR 2010; 195:677-686"CTC increased the odds of identifying high risk lesions by 78%. CTC should be considered as an alternative to optical colonoscopy for colorectal cancer screening or as a onetime procedure to identify significant treatable intracolonic and extracolonic lesions."
Extracolonic Findings on CT Colonography Increases Yield of Colorectal Cancer Screening
Veerappan GR et al
AJR 2010; 195:677-686- 2,277 patients had CTC
- Extracolonic findings in 1037 patients (46%)
- 787 were insignificant and 240 significant
- Significant findings resulted in 280 radiology procedures and 19 surgeries
- Total additional cost of radiology was $113,179 or $50 extra per patient "Among the 57 patients who had experienced both procedures, 95% (n=54) preferred CTC."
CT Colonography May Improve Colorectal Cancer Screening Compliance
Moawad FJ et al
AJR 2010; 195:1118-1123- Other identified reasons for CTC Selection
- Personal recommendation
- Ability to detect extracolonic pathology
- Poor previous colonoscopy experience
- Incomplete colonoscopy in the past "Two hundred fifty consecutive average-risk patients undergoing CRC screening completed a survey that assessed reasons for choosing CTC in lieu of colonoscopy, compliance with CRC screening if CTC was not offerred, and which of the two tests they preferred."
CT Colonography May Improve Colorectal Cancer Screening Compliance
Moawad FJ et al
AJR 2010; 195:1118-1123- Why do we do Colon Cancer screening?
- The prevalence of adenomas in the general population is 30-50% and increases with age
- The vast majority of adenomas are <1cm and these lesions have about a 1% likelihood of containing invasive cancer.
- Only 1-3% of adenomas ever progress to cancer "Our study shows that the CAD-related increase in sensitivity for lesions 6 mm or larger renders CT colonography screening both clinically effective and cost effective for inexperienced and experienced readers, substantially raising the CRC prevention rate with only a modest increase in program costs."
Impact of Computer-aided Detection on the Cost-effectiveness of CT Colonography
Rgge D et al.
Radiology 2009; 250:488-497"The addition of CAD to CT colonography screening imroves the CRC prevention rate, resulting in advantageous cost-effectivemess for screening."
Impact of Computer-aided Detection on the Cost-effectiveness of CT Colonography
Rgge D et al.
Radiology 2009; 250:488-497Kim et al, NEJM 2007;357:1403-1412
Total number of polyps removed
- 561 in CTC group
- 2434 in OC group
Perforations
- 7 in OC group, 4 requiring surgery
- 0 in CTC group
Conclusion: “These findings support the use of CTC as a primary screening test before therapeutic OC.”Kim et al, NEJM 2007;357:1403-1412
Primary CTC in 3120 adults vs. OC in 3163 adults
- CTC 123 advanced neoplasia
--14 invasive cancers
- OC 121 advanced neoplasic
--4 invasive cancers
Referral at CTC to OC was 7.9% (lesions > 6mm)
- Patients with 1 or 2 small polyps (6-9mm) were offered option of CT surveillance- ACRIN Summary
- CTC screening identified 90% of patients with adenomas or cancers, >10mm
- Extracolonic abnormalities reported were similar to other studies
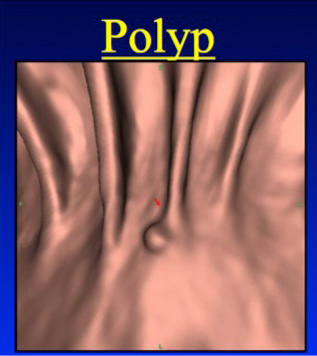
--- need management algorithms - Polyps
- 1629 patients had no polyps
- 2141 patients had no polyps >5mm
- 512 had at least 1 polyp, the largest < 5mm
- 258 patients with with polyps 5-9mm132 patients with polyps > 10mm
- 7 lesions were malignant
---- 2- 10mm,1- 15mm, 2-25mm, 1-55mm, 1-100mm
- ACRIN CTC Technique
Automated colonic insufflation with CO2
- Supplemented with manual room air if needed
1mg glucagon, sub Q -92%
- Administered 7-15 minutes prior to the study, unless contraindicated or declined by the participant - ACRIN CTC Technique
- Exams randomly assigned to be read independently with the use of either a primary 2D or primary 3D search method
- Radiologists confidence that each finding was a polyp was rated on a scale 0-5.
- Radiologists recorded all lesions 5mm or more in diameter. - ACRIN CTC Interpretation
CTC software used for interpretation
- Vital Images
- General Electric
- Siemens
- Viatronix
- TeraRecon - Colon: ACRIN CTC Technique
MDCT Protocol
- Collimation 0.5-1.0mm,
- Pitch 0.98 to 1.5
- Matrix 512 x 512
- Field of view to fit patient
- 50 mAs, 120kV
- Standard reconstruction algorithm
- Prone and supine acquisition
- 1.0-1.25mm slices reconstructed at 0.8mm intervals
- ACRIN CTC Technique
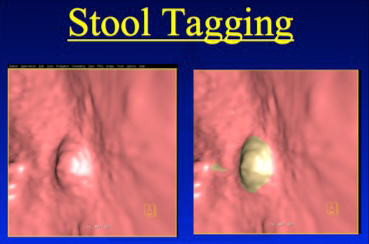
Stool and liquid tagging
-Barium sulfate - 98% Iodinated contrast - 94%-
Laxative purgation
- Polyethylene glycol - 40%
- Sodium phosphate solution - 55%
- Magnesium citrate- 4%
- Other -1%
- Radiologist Training
- All radiologists required to complete a qualifying examination in which they achieved a detection rate of 90% or more for polyps 10 mm or larger
- Of 20 radiologists who met the initial entry criteria, the 15 with the highest scores on the qualifying exam were invited to participate in the study. - National CTC Trial-ACRIN
Accuracy of CT Colonography for Detection of Large Adenomas and CancersC. Daniel Johnson, et al
NEJM, 2008;359:1207-17. - Study population
- 2600 asymptomatic study participants, age 50 or older
- 15 centers
- Complete data were available in 2531 (97%) - Pickhardt, N Engl J Med 2003;349:2191-2200
Difference in Pickhardt study
--Patient population
-- Primary 3D evaluation
-- Stool and liquid tagging with electronic subtraction
-- MDCT (4 and 8 row) - Pickhardt, N Engl J Med 2003;349:2191-2200
SensitivityPolyp sizeVCOC>10mm94%88%8mm94%92%6mm89%92% Pickhardt, N Engl J Med 2003;349:2191-2200
- 1233 Asymptomatic Adults
- Average risk, > 50 y.o.
- Same day VC and optical colonoscopy
- Adenomas > 10mm
--- Sensitivity (by patient) 94%
--- Specificity (by patient) 96%
--- Sensitivity (by lesion) 92%
Colon: CT Colonography
- Fast, visualizes the entire colon
- Less invasive, less morbidity (perforation risk 2:20,000)
- Hope that compliance will be increased
- Reduced cost compared to colonoscopy
- Better tolerated by patients than conventional colonoscopy (Svensson, Radiology 2002) (Glueker, Radiology 2003)
- Better tolerated than DCBE (Glueker, Radiology 2003)"CTC showed a high sensitivity for nonpolypoid stage Tis and T1 adenocarcinomas 10 mm or greater in width despite the limited sensitivity for nonpolypoid adenomatous lesions, when performed using cathartic preparation and fecal tagging."
Sensitivity of CT Colonography for Nonpolypoid Colorectal Lesions Interpreted by Human Readers and With Computer Aided Detection
Park SH et al.
AJR 2009; 193:70-78- "Increasing number of CAD false positive marks did not adversely influence correct reader study classicification or diagnostic confidence, although reporting times did increase."
CT Colonography and Computer Aided Detection:Effect of False Positive Results on Reader Specificity and reading Efficiency in a Low Prevalence Sceening Population
Taylor SA et al.
Radiology 2008;247:133-140 - "CT colonography has the potential to become an accepted technique for evaluation of the nonvisualized part of the colon after incomplete colonoscopy, and it can increase the diagnostic yield of masses and clinically important polyps in this part of the colon."
CT Colonography in 546 Patients with incomplete Colonoscopy
Copel L et al.
Radiology 2007; 244:471-478 - "CT colonography after incomplete colonoscopy has per-patient and per-lesion positive predictive values of 90.9% and 91.7%, respectively, for masses (lesions >20mm) and 64.7% and 70%, respectively, for polyps of 10 mm or larger."
CT Colonography in 546 Patients with incomplete Colonoscopy
Copel L et al.
Radiology 2007; 244:471-478 - "Primary 2D CTC is less sensitive than primary 3D CTC for polyp detection in low-prevalence screening cohorts. The disappointing 2D sensitivity in this study was very similar to results obtained with primary 2D evaluation in previous CTC trials."
Primary 2D versus primary 3D polyp detection at screening CT colonography
Pickhardt PJ et al.
AJR 2007 Dec; 189(6):1451-1456 - Conclusions: CT virtual colonoscopy with the use of a three-dimensional approach is an accurate screening method for the detection of colorectal neoplasia in asymptomatic average-risk adults and compares favorably with optical colonoscopy in terms of the detection of clinically relevant lesions."
Computed Tomographic Virtual Colonoscopy to Screen for Colorectal Neoplasia in Asymptomatic Adults
Pickhardt PJ et al.
N Eng J Med 2007 Dec 349:2191-2200 - "The sensitivity of virtual colonoscopy for adenomatous polyps was 93.8 percent for polyps at least 10 mm in diameter, 93.9 percent for polyps at least 8 mm in diameter, and 88.7 percent for polyps at least 6 mm in diameter. The sensitivity of optical colonoscopy for adenomatous polyps was 87.5 percent, 91.5 percent, and 92.3 percent for the three sizes of polyps, respectively. The specificity of virtual colonoscopy for adenomatous polyps was 96.0 percent for polyps at least 10 mm in diameter, 92.2 percent for polyps at least 8 mm in diameter, and 79.6 percent for polyps at least 6 mm in diameter. Two polyps were malignant; both were detected on virtual colonoscopy, and one of them was missed on optical colonoscopy before the results on virtual colonoscopy were revealed."
Computed Tomographic Virtual Colonoscopy to Screen for Colorectal Neoplasia in Asymptomatic Adults
Pickhardt PJ et al.
N Eng J Med 2007 Dec 349:2191-2200 - "The sensitivity of virtual colonoscopy for adenomatous polyps was 93.8 percent for polyps at least 10 mm in diameter, 93.9 percent for polyps at least 8 mm in diameter, and 88.7 percent for polyps at least 6 mm in diameter. The sensitivity of optical colonoscopy for adenomatous polyps was 87.5 percent, 91.5 percent, and 92.3 percent for the three sizes of polyps, respectively. The specificity of virtual colonoscopy for adenomatous polyps was 96.0 percent for polyps at least 10 mm in diameter, 92.2 percent for polyps at least 8 mm in diameter, and 79.6 percent for polyps at least 6 mm in diameter.."
Computed Tomographic Virtual Colonoscopy to Screen for Colorectal Neoplasia in Asymptomatic Adults
Pickhardt PJ et al.
N Eng J Med 2007 Dec 349:2191-2200 - Compared with the conventional 2D colonic polyp detection method, primary 3D interpretation with use of virtual dissection software for CT colonography revealed comparable per-polyp (77% and 69% for two readers) and per-patient (77% and 73% for two readers) sensitivities and comparable per-patient specificity (99% and 89% for two readers) for the detection of polyps 6 mm in diameter or larger and involved a shorter interpretation time.
Two versus three dimensional colon evaluation with recently developed virtual dissection software for CT
Kim SH et al.
Radiology 2007 Sep;244(3):852-64 - "If CT colonography shows no abnormality, follow up screening in 5 years is recommended."
Significance of Missed Polyps at CT Colonography
Macari M et al.
AJR 2004;183:127-134 - "If CT colonography detects a lesion measuring 6 mm or more, endoscopy and poypectomy should be offered unless contraindicated."
Significance of Missed Polyps at CT Colonography
Macari M et al.
AJR 2004;183:127-134 - Virtual Colonoscopy: Techniques
- Patient Preparation: 24 hr prep
- Fleet 1 Prep
- 500 ml of 2.1% barium contrast (Scan C, Lafayette Pharmaceuticals)
- 120 ml gatrograffin - "CT colonography has no significant cardiovascular effect other than spasmolytic induced tachycardia. Endoscopy- and colonoscopy in particular- causes cardiovascular effects that are largely related to sedation. CT colonography is less painful than colonoscopy and is comparible to flexible sigmoidoscopy."
Cardiovascular Effects at Multidetector Row CT Colonography Compared with Those at Conventional Endoscopy of the Colon
Taylor SA et al.
Radiology 2003; 229:782-790 - "Lower dose multidetector helical CT colonography ensures substantial dose reduction while maintaining excellent sensitivity for detection of colorectal carcinomas and polyps larger than 6 mm in diameter."
Detection of Colorectal lesions: Lower-Dose Multidetector Row helical CT Colonography Compared with Conventional Colonoscopy
Iannaccone R et al.
Radiology 2003; 229:775-781 - "Specificity improved for both readers with thin sections (1.25 mm sections reconstructed every 1 mm as opposed to 5 mm sections reconstructed every 2 mm), with no difference in sensitivity."
CT Colonography Data Interpretation: Effect of Different Section Thicknesses-Preliminary Observations
Lui YW et al.
Radiology 2003; 229:791-797 - "Polyps can be found in 50% of adults at 50 years old and 70% by 70 years. 50% of polyps in the average adult colon are only hyperplastic normal tissue."
Virtual Colonoscopy for Colon Cancer Screening: Further Reflections on Polyps and Politics
ferrucci JT
AJR 2003;181:795-797