State of the Art 3DCT Angiography Assessment of Upper Extremity Trauma: Pearls, Pitfalls, and Study Design Optimization
State of the Art 3DCT Angiography Assessment of Upper Extremity Trauma: Pearls, Pitfalls, and Study Design Optimization |
Objectives
|
Introduction
|
Epidemiology and Etiology
|
Management Scenarios with so-called hard signs of vascular injury usually require immediate surgical exploration and appropriate treatment, such as repair or bypass: 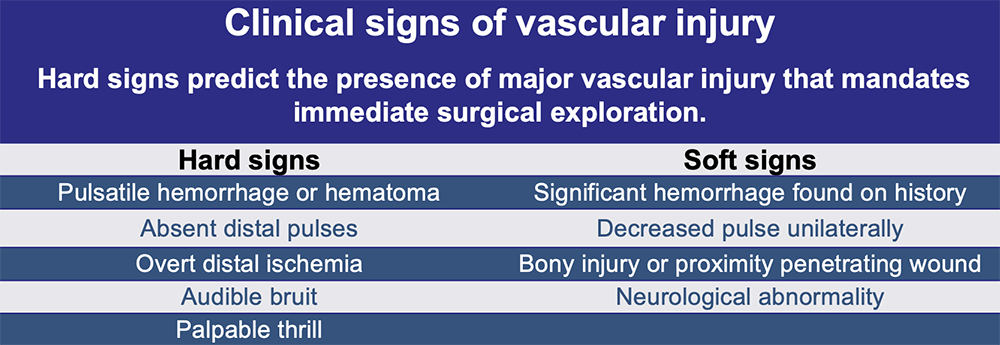 |
Top 4 indications for MDCTA
|
The Algorithm 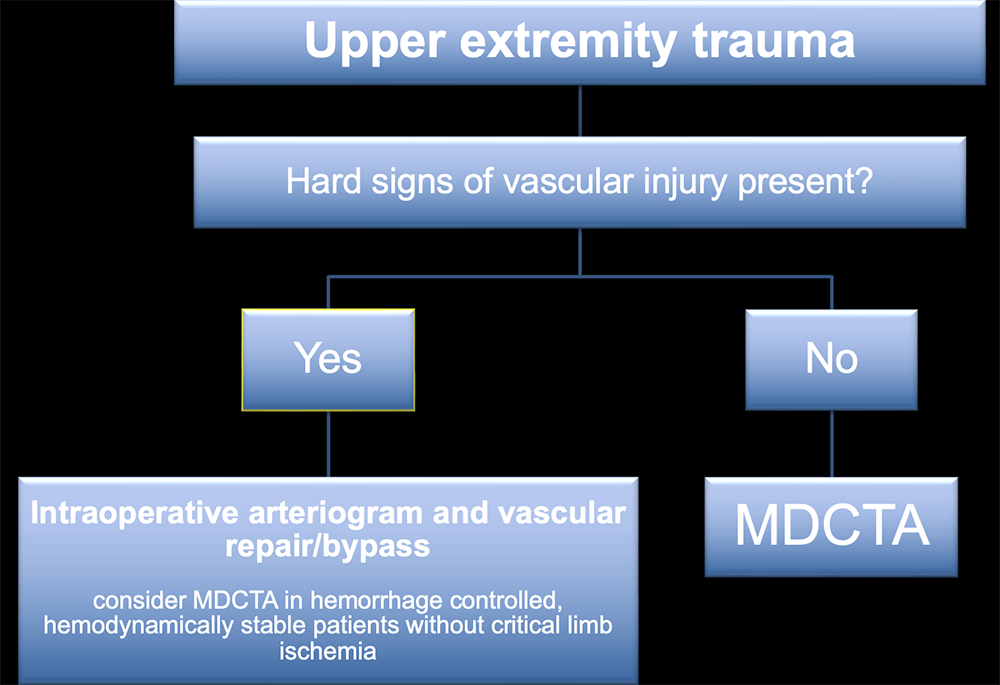 |
Optimization of MDCT acquisition parameters and low-dose techniques
|
64 Slice MDCT angiography protocols 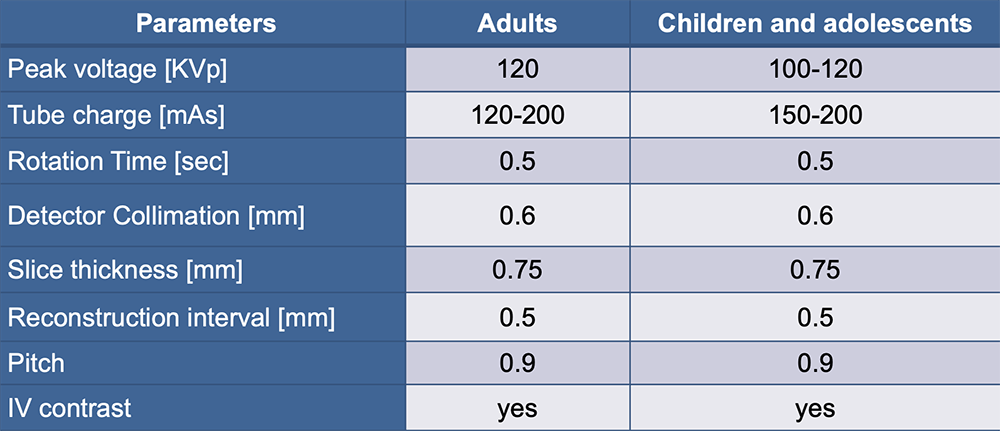 |
Metal artifact reduction Reducing artifacts from high-density foreign matter:
Artifacts may also be substantially reduced by Dual Energy CT based high energy extrapolation algorithms. |
MDCTA versus Digital Subtraction Angiography 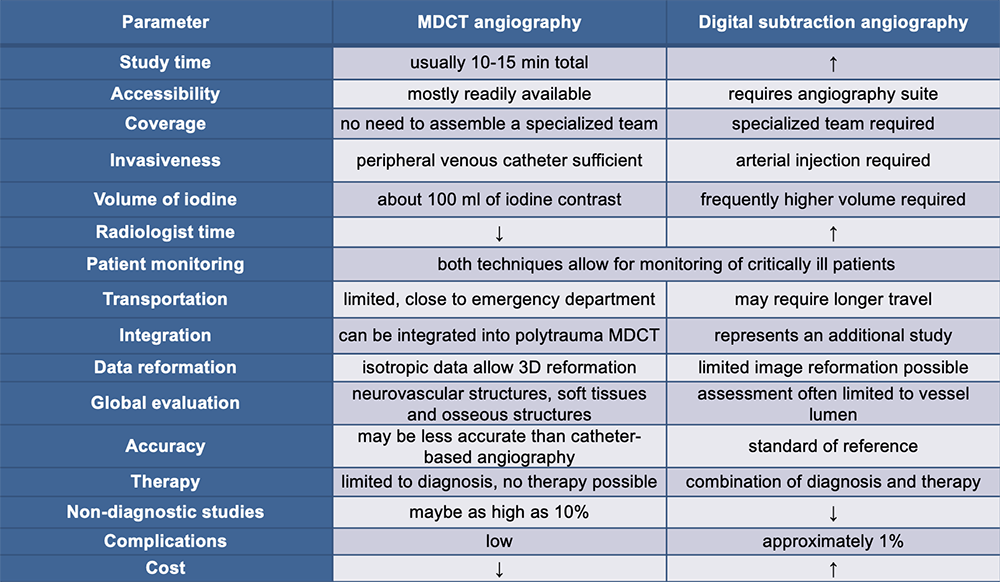 |
Pertinent vascular MDCT angiography anatomy 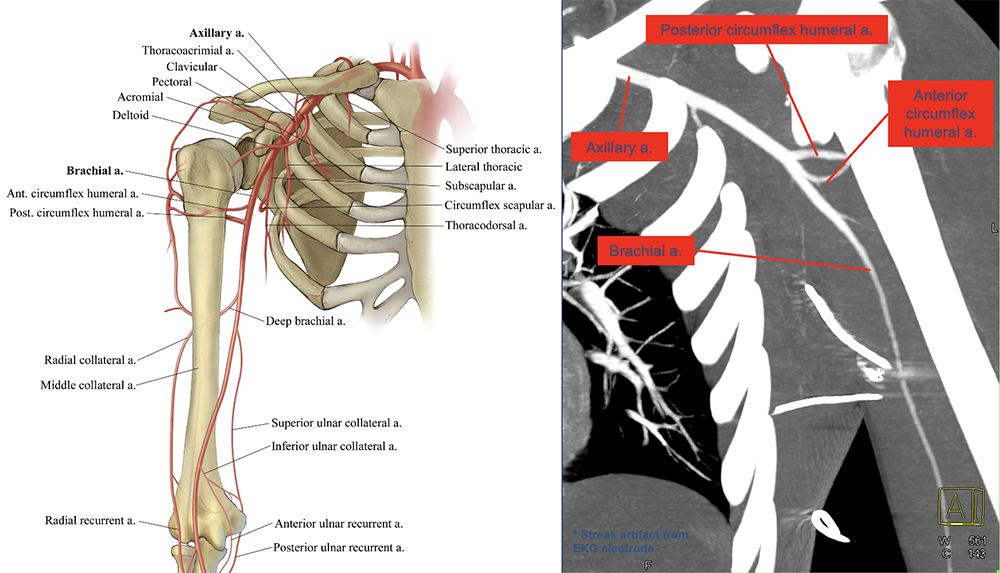 |
Pertinent vascular MDCT angiography anatomy 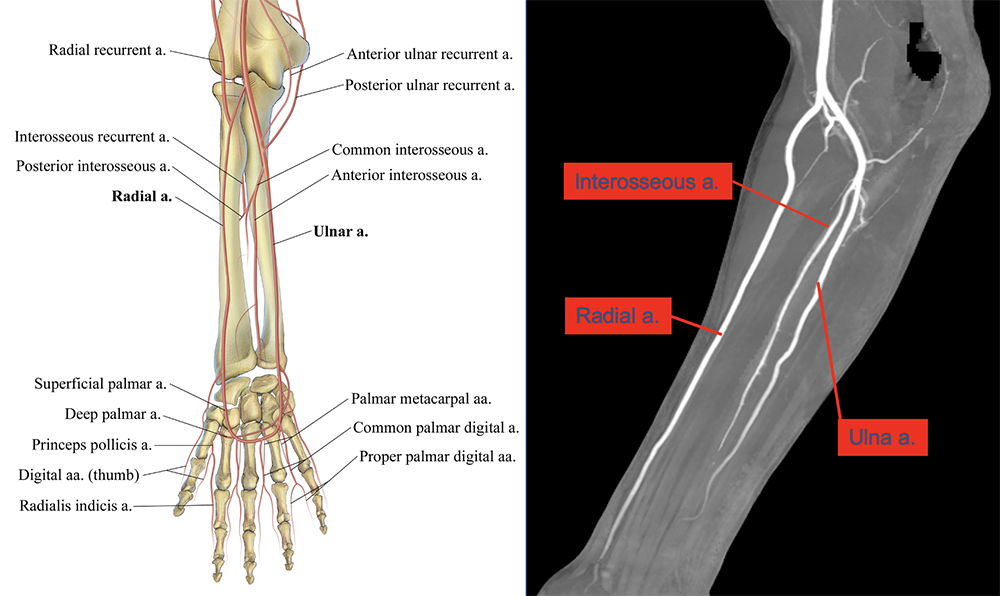 |
3D visualization 3D mapping of MDCTA data allows for virtual visual inspection, simulated classic catheter digital subtraction angiogram, provides the capability to display tissue muscle, soft tissues, and bone, and segmentation capabilities for virtual bone removal, which may be required for maximum intensity projection and volume rendering technique. 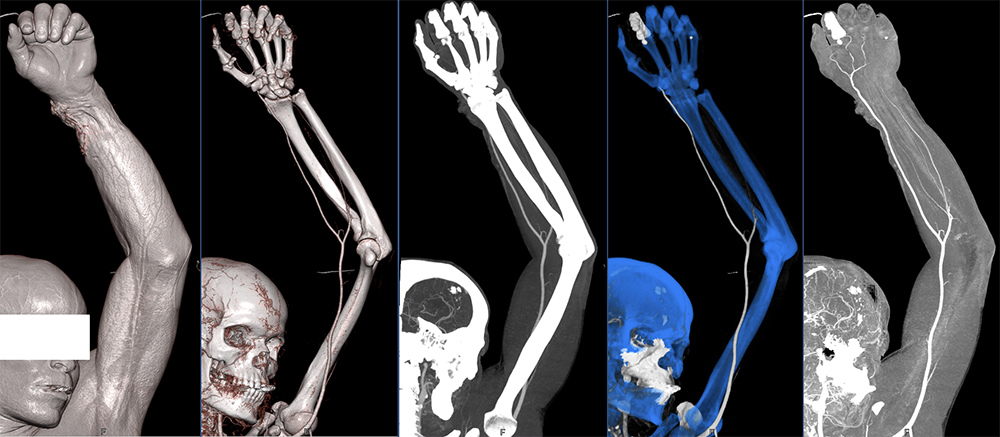 |
MDCTA of vascular injury Findings of arterial injuries include:
|
Active extravasation Active extravasation is caused by disruption of all layers of the vessel wall, which can be partial or involve the entire circumference of the vessel. MDCTA is helpful for the differentiation of ongoing hemorrhage versus hematoma without active bleeding. Clotted hematomas without active hemorrhage are typically hyperdense and show no signs of iodine-contrast accumulation. Acute hemorrhage is demonstrated by the accumulation of iodine contrast material inside a hematoma or in soft tissues. MDCTA is especially helpful in differentiating active hemorrhage of peripheral arterial branches, which may be treated with conservatively from active hemorrhage of a major artery, which are more likely to require surgery. Illustration demonstrates active arterial extravasation with disruption of all layers and partially clotted hematoma. 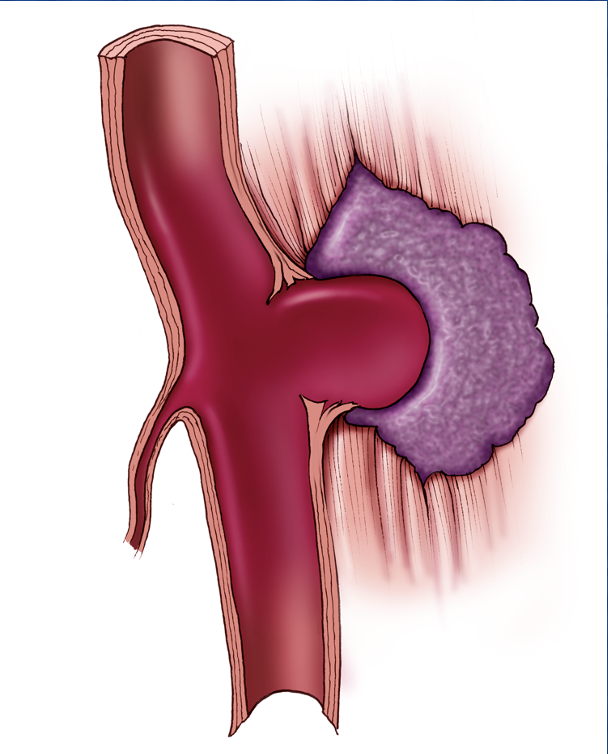 |
Active extravasation Soft tissues MDCTA and 3DCT images following stab wound trauma of the left chest demonstrate an arterial extravasation (red arrows) of the left pectoralis major of a small branch of the thoracoacromial. The axillary artery is intact (yellow arrows). 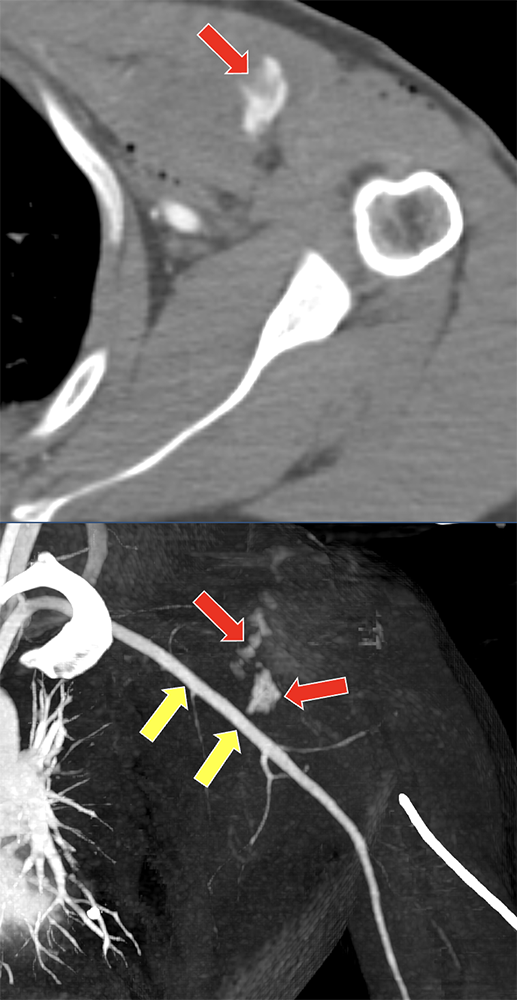 |
Active extravasation Small arterial branches MDCTA and 3DCT images following blunt chest trauma demonstrate a soft tissue hematoma involving the left latissimus dorsi muscle (red arrow) with small foci of active hemorrhage originating from branches of the circumflex scapular artery (yellow arrows). Data were acquired with elevated left arm.  |
Active extravasation Small arterial branches 3D CTA images following gun shot injury of the proximal left upper extremity demonstrates the bullet entry (red arrow) and focal active arterial extravasation of a branch of the profunda brachii artery (yellow arrows). 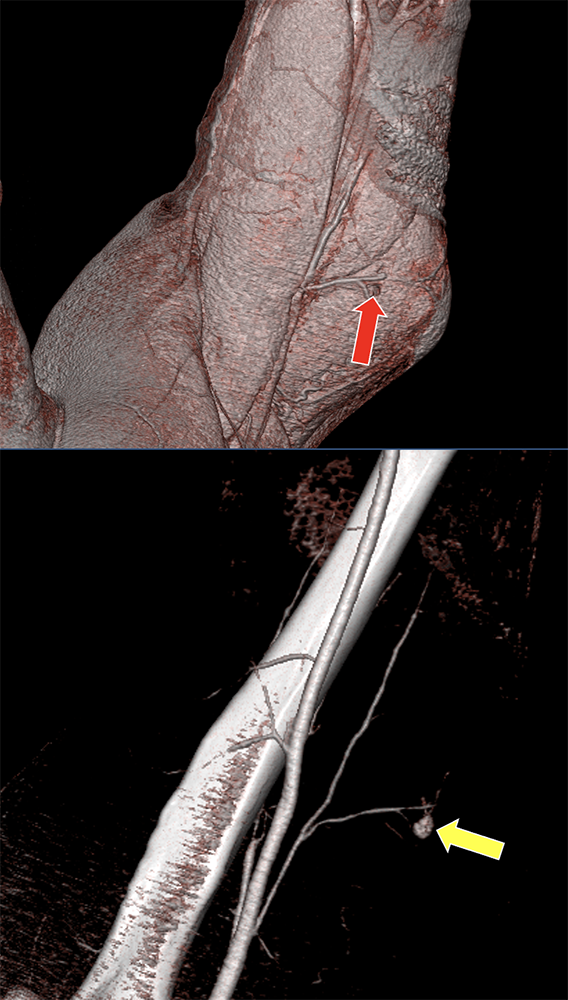 |
Active extravasation Small arterial branches with soft tissue laceration 3D CTA images of a mangled right upper extremity* demonstrate a soft tissue laceration of the elbow region with active arterial extravasation (red arrows) of branches of the profunda brachii artery (yellow arrows). * defined as high energy transfer and/or crush injury resulting in some combination of injuries to artery, bone, tendon, nerve and/or soft tissue 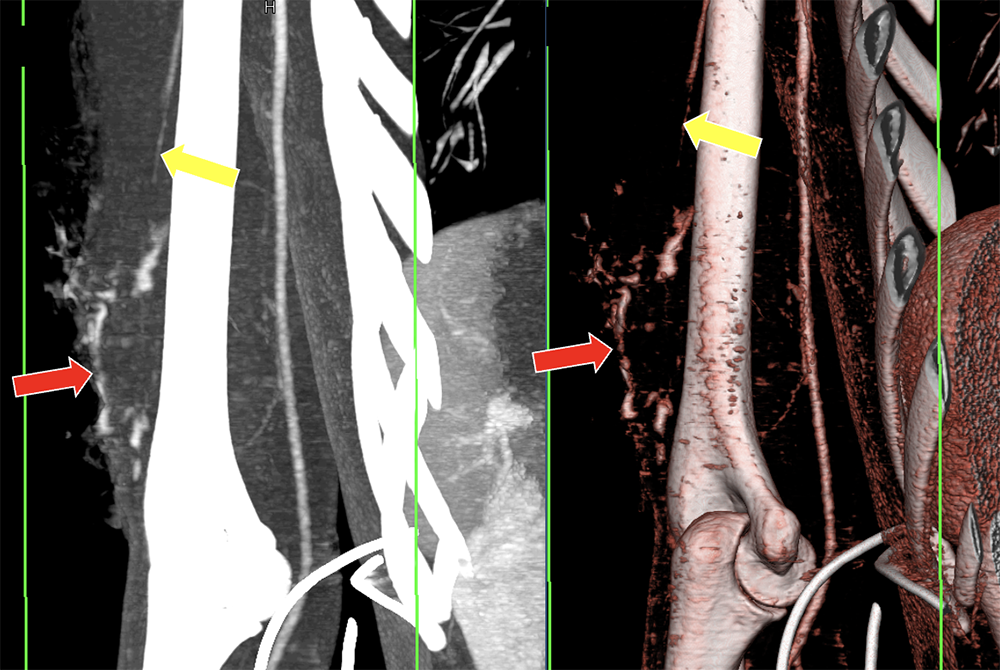 |
Active extravasation Transection MDCTA and 3DCT images following penetrating injury of the right axillary region demonstrate active hemorrhage originating from the axillary artery (yellow arrows) with no apparent contrast enhancement distally (red circles), representing a surgically proven transection. 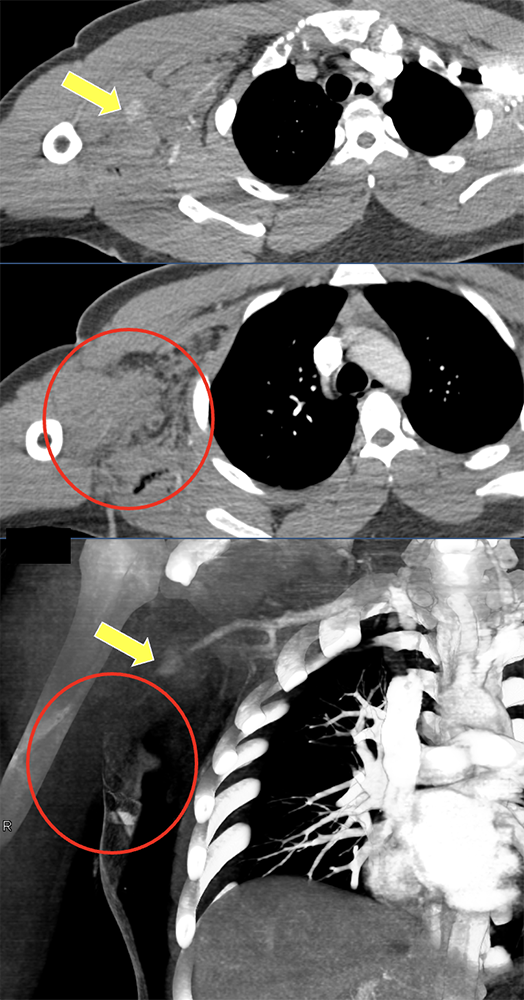 |
Active extravasation Transection 3D CTA images of a mangled upper extremity* show soft tissue laceration (yellow arrow) and underlying traumatic transection of the proximal brachial artery (red arrow) with absent blood flow distally. * defined as high energy transfer and/or crush injury resulting in some combination of injuries to artery, bone, tendon, nerve and/or soft tissue 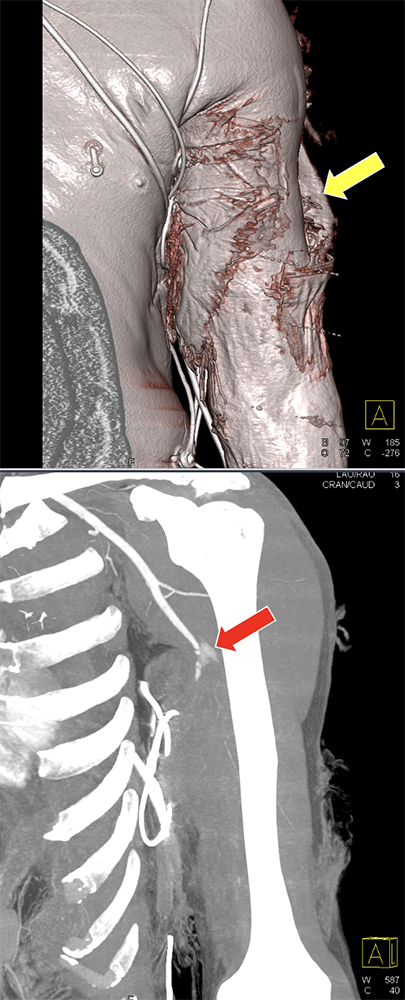 |
Pseudoaneurysm Pseudoaneurysm is caused by incomplete disruption of the layers of the arterial wall. The occurrence of a pseudoaneurysm may be delayed or it may manifest as a contained hematoma during the healing phase of a vascular injury. Illustration demonstrates incomplete disruption of the arterial wall and the sequence of development of a pseudoaneurysm (box). 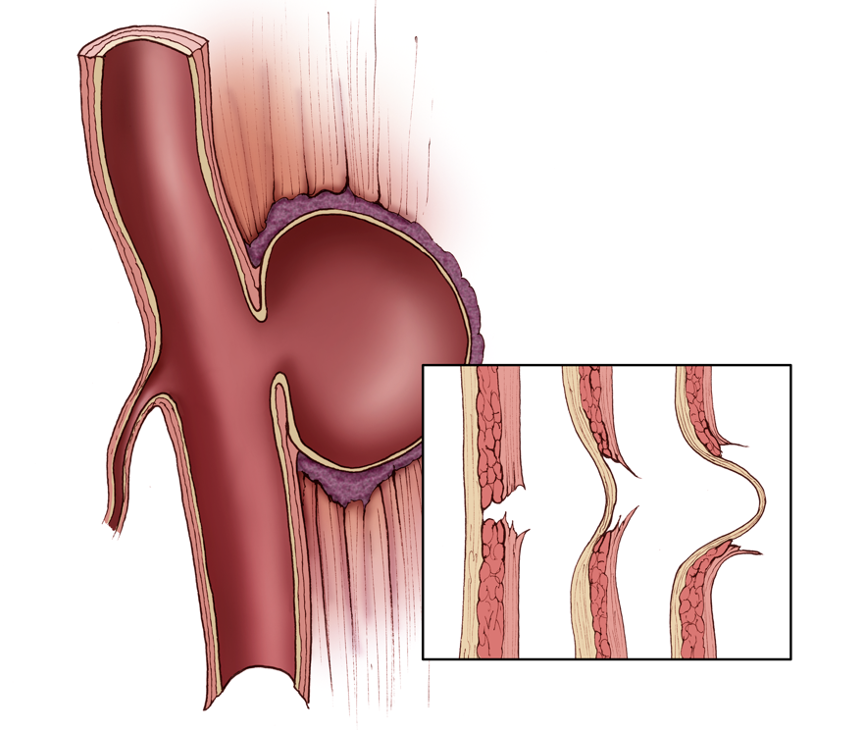 |
Pseudoaneurysm 3D MDCTA image in a patient following gun short trauma shows a comminuted fracture of the right scapula (yellow arrow) and a traumatic pseudoaneurysm of the right axillary artery (right arrow) in the trajectory of the bullet. 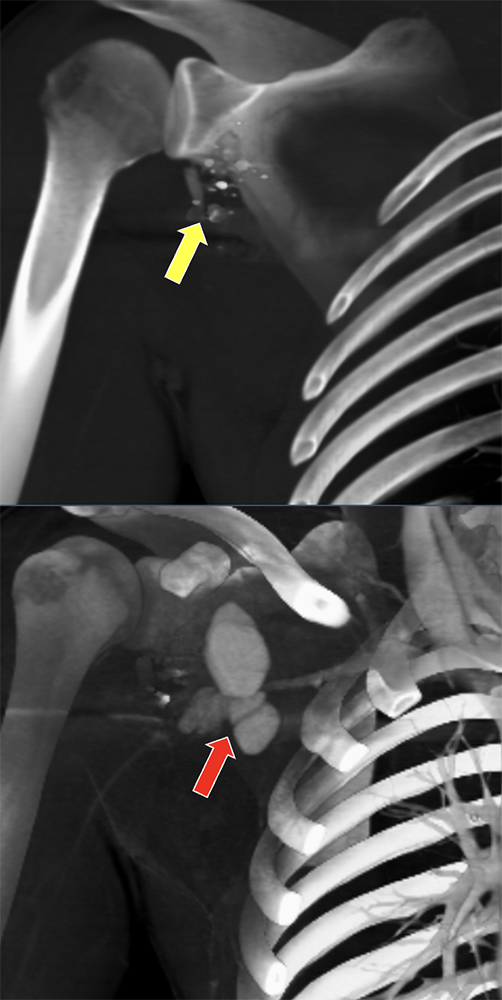 |
Pseudoaneurysm 3D MDCTA images in a patient after nail gun injury of the left elbow region demonstrates a pseudoaneurysm of a small branch of the radial artery (arrows). 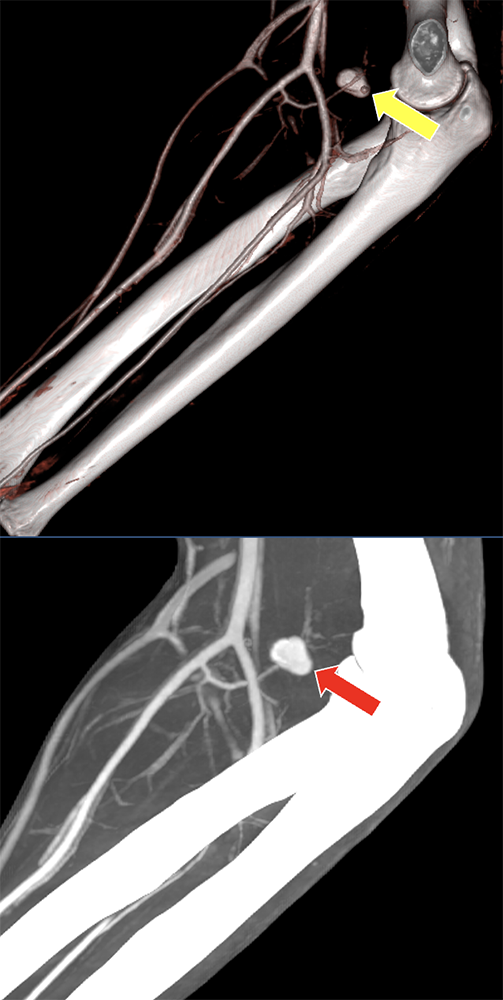 |
Vascular occlusion and spasm Luminal narrowing and occlusion can be due to severe vasospasm, dissection, injury of the intima with thrombus formation, and external compression. Post-traumatic vasospasm presents as reactive, transient luminal narrowing. In cases of vasospasm, signs of arterial insufficiency resolve over time. Dissection may present as narrowing of the vessel lumen and may not be differentiated with certainty on MDCTA. In such cases, catheter-based angiography may be helpful and close clinical follow-up is indicated. MDCTA follow-up may be helpful for further differentiation as well. Illustrations of arterial vasospasm (left) and arterial dissection (right) with inlay schemes demonstrating the similarity of the appearance of the contrast opacified lumen. 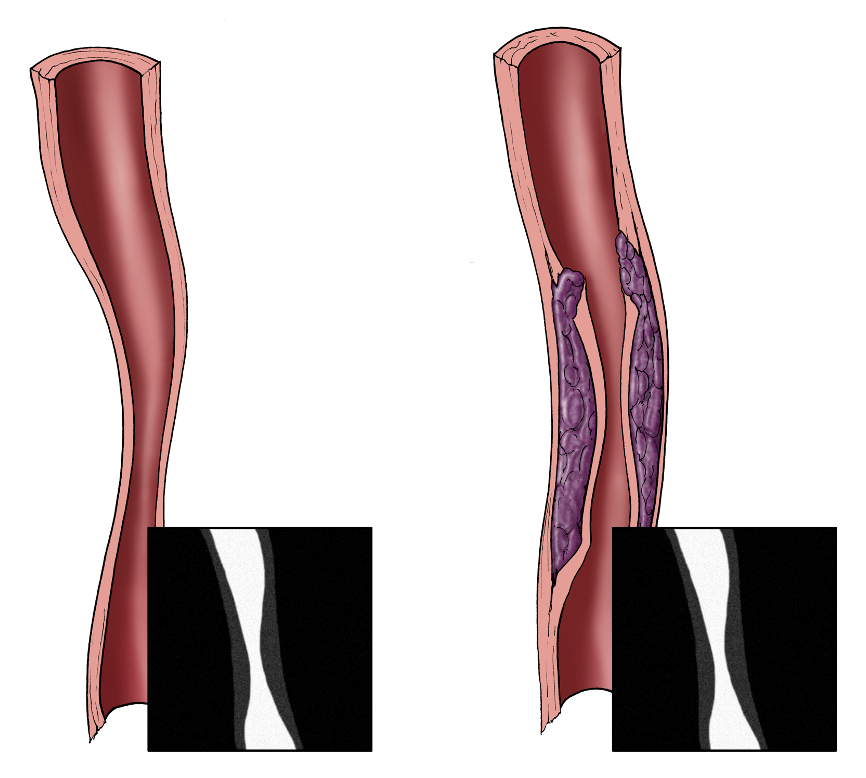 |
Vascular occlusion 3D CTA images of a mangled forearm show a large soft tissue laceration (red arrow) and underlying traumatic occlusion of the ulnar artery (yellow arrow) without distal reconstitution. There radial artery (blue arrow) is preserved. 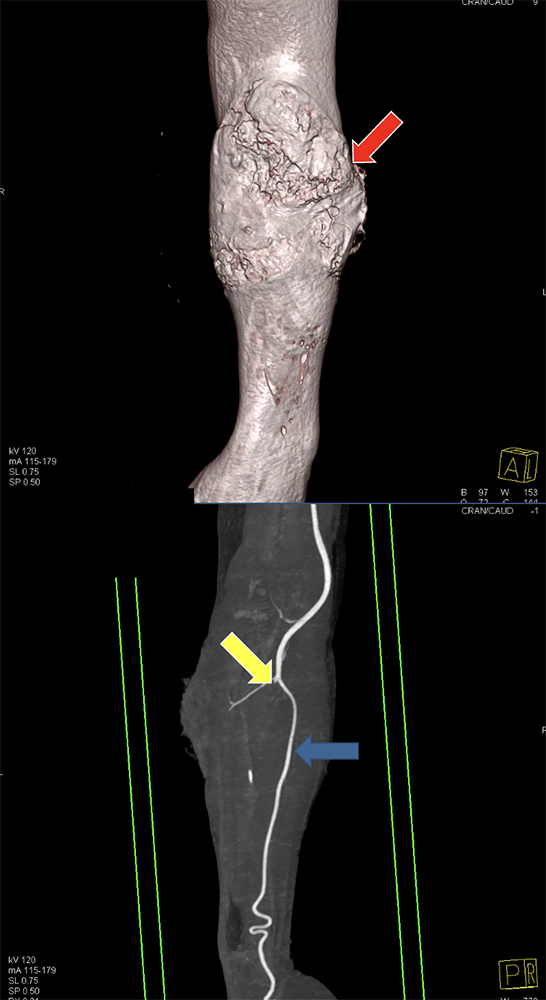 |
Vascular occlusion 3D CTA images following blunt trauma of the right elbow region show a filling defect in the right ulnar artery (arrows) with distal reconstitution of the vessel. Surgical exploration demonstrated disruption of the intima with thrombus formation. 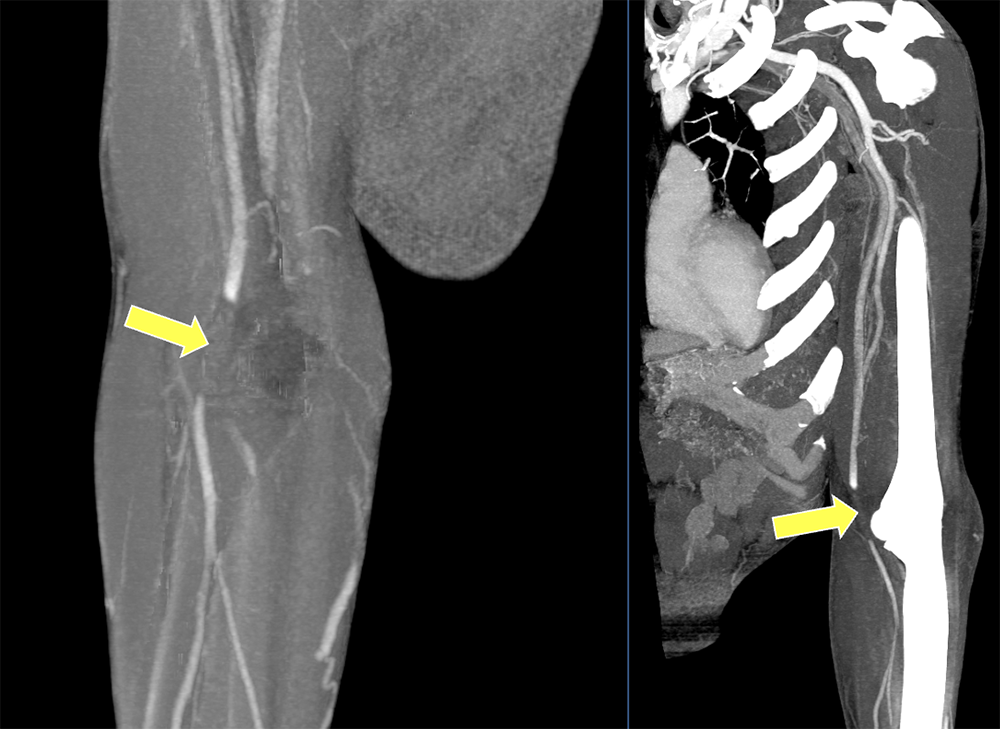 |
Spasm 3D CTA images of a mangled left forearm show a soft tissue laceration (red arrow) and segmental narrowing of the ulnar artery (yellow arrow) and radial artery (blue arrows) with distal reconstitution due to severe vasospasm, which resolved over time. 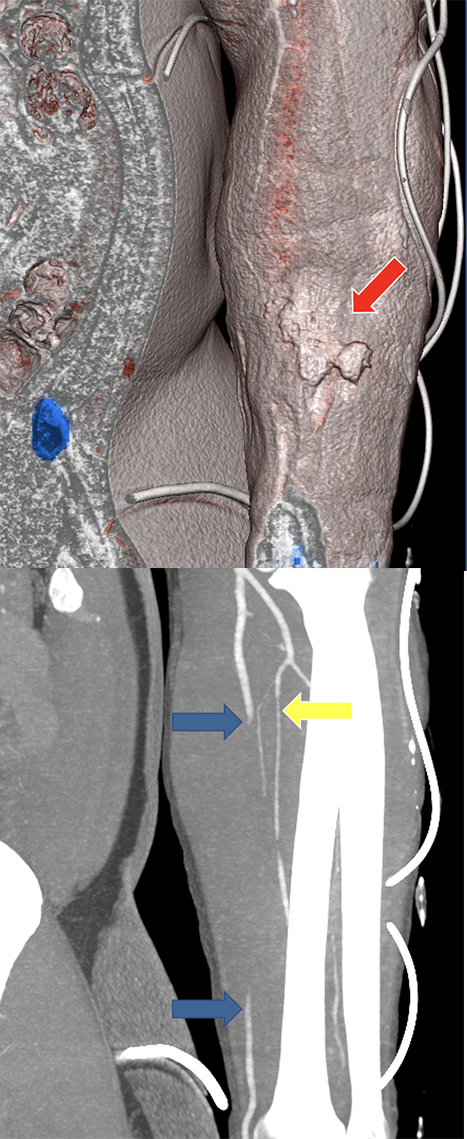 |
Early venous contrast opacification Early venous contrast opacification can be an indirect sign of a traumatic arteriovenous fistula or can be due to trauma-related hyperemia. Arteriovenous fistulas are abnormal communications with shunting of blood from an artery to a vein that occur after simultaneous damage of the two adjacent vessels. Common causes include penetrating trauma from gunshot and stab wound. Illustrations of an arteriovenous gunshot injury with resulting fistula and abnormal shunting of arterial blood (arrow) into the vein (blue vessel) explaining early venous contrast opacification. 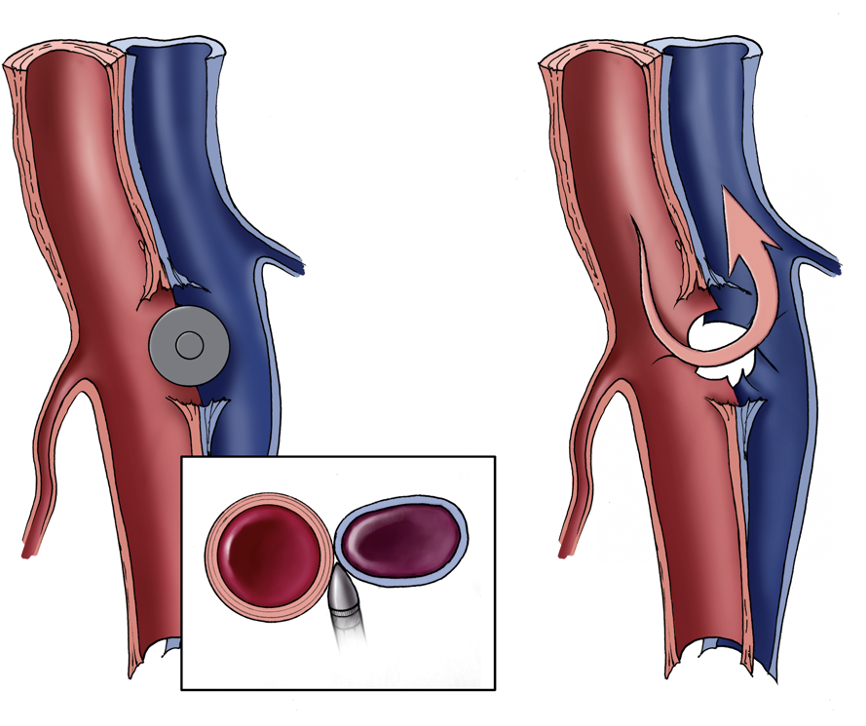 |
Associated injury 3D CTA image of a penetrating trauma of the left shoulder demonstrates active hemorrhage (arrow) originating from the cephalic vein. 3D CTA image of a mangled right forearm demonstrates a comminuted ulnar shaft fracture (arrow). 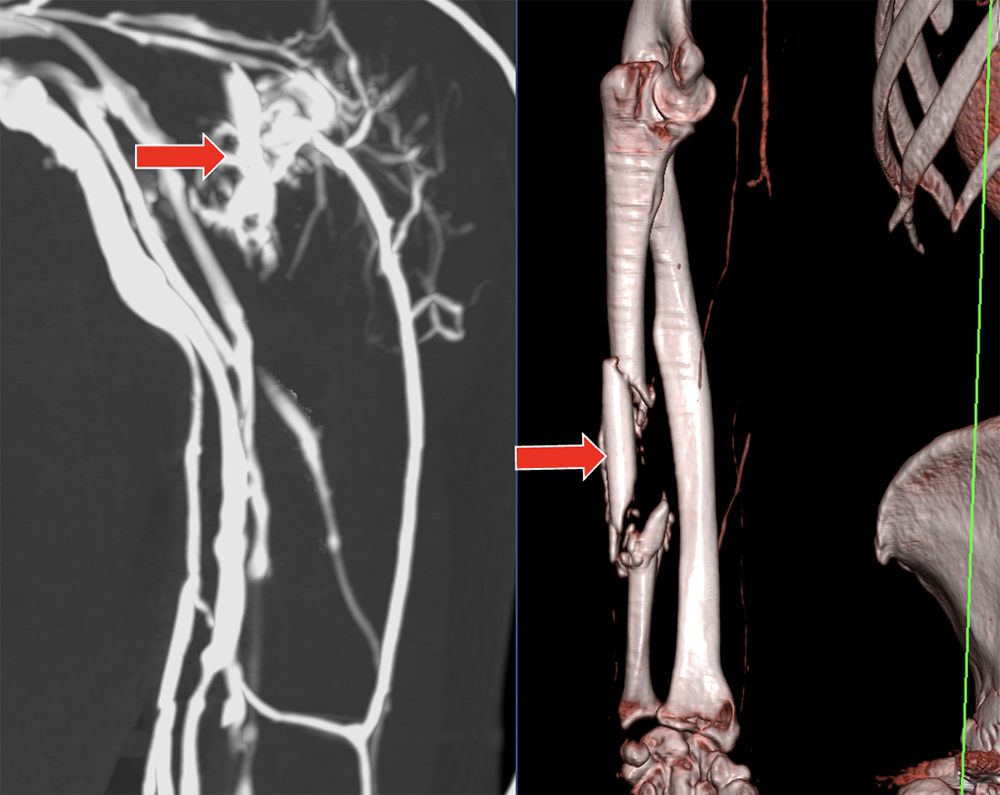 |
Rib Fractures 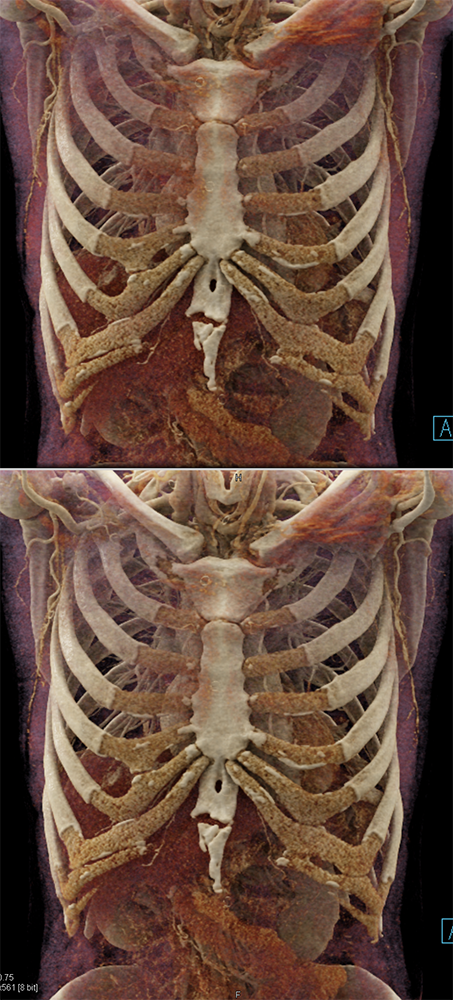 |
 |
 |
Pearls
|
Pitfalls
|
Summary
|