|
-- OR -- |
|
- • Serial cardiac troponin (cTn) biomarkers, preferably high-sensitivity cardiac troponin (hs-cTn), are useful for rapid detection and exclusion of myocardial injury (class 1 strength of recommendation; level B-NR quality of evidence [nonrandomized]).
• Structured risk assessment and evidence-based clinical decision pathways(CDPs) should be used to facilitate disposition and guide diagnostic evaluation (class 1 strength; level B-NR quality).
• Low-risk patients with acute or stable chest pain may be discharged home without urgent cardiac testing (class 2a strength for acute chest pain, class 1 strength for stable chest pain; level B-R quality [randomized]).
Evaluation and Diagnosis of Chest Pain
David G. Beiser, Adam S. Cifu, Jonathan Paul
JAMA Published online July 1, 2022 - • For intermediate-risk patients with acute chest pain and no known coronary artery disease (CAD), coronary computed tomographic angiography (CCTA) is useful for exclusion of atherosclerotic plaque and obstructive CAD (class I strength; level A quality).
• For intermediate-risk patients with acute chest pain and no known CAD, functional testing (eg, exercise electrocardiography, stress echocardiography, stress positron emission tomography/single-photon emission computed tomography myocardial perfusion imaging, or stress cardiac magnetic resonance) is useful for diagnosis of myocardial ischemia (class I strength; level B-NR quality [nonrandomized]).
Evaluation and Diagnosis of Chest Pain
David G. Beiser, Adam S. Cifu, Jonathan Paul
JAMA Published online July 1, 2022 - • For intermediate-risk patients with acute chest pain and no known CAD, functional testing (eg, exercise electrocardiography, stress echocardiography, stress positron emission tomography/single-photon emission computed tomography myocardial perfusion imaging, or stress cardiac magnetic resonance) is useful for diagnosis of myocardial ischemia (class I strength; level B-NR quality[nonrandomized]).
• Clinically stable patients presenting with chest pain should be included in decision-making. Information about risk of adverse events, radiation exposure, costs, and alternative options should be provided to facilitate the discussion.
Evaluation and Diagnosis of Chest Pain
David G. Beiser, Adam S. Cifu, Jonathan Paul
JAMA Published online July 1, 2022
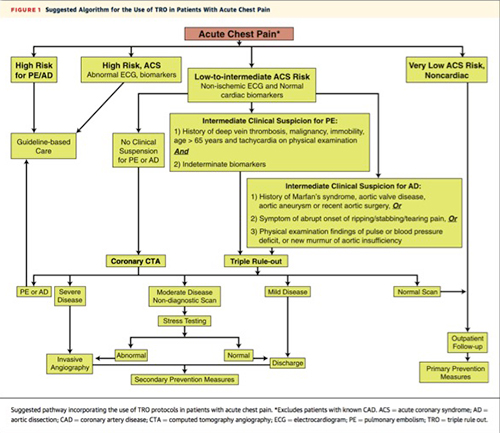
- “TRO was associated with slightly higher yield of PE and AD, specifically in the emergency department. This benefit comes with higher nondiagnostic image quality, radiation, and contrast doses. Although TRO may be of value in selected patients, its indiscriminate use is not warranted. The appropriate use of TRO needs to be further defined.”
Triple Rule Out Versus Coronary CT Angiography in Patients With Acute Chest Pain
Burris II, AC et al.
(J Am Coll Cardiol Img 2015;8:817–25 - “Subsequently, Rowe and colleagues discussed cinematic rendering as a new 3D method aimed at enhancing the display of volumetric data acquired on CCT. They presented an example of a 50 year old man who presented with chest pain and had a 50% stenosis in the proximal left anterior descending artery, showing the utility of cinematic rendering in fully delineating the relative position of other cardiac structures.”
The Journal of Cardiovascular Computed Tomography year in review - 2018
Al’Aref SJ et al.
Journal of Cardiovascular Computed Tomography (in press)
- OBJECTIVE. The objective of the present study is to quantify the diagnostic yield of triple-rule-out (TRO) CT for the evaluation of acute chest pain in emergency department patients.
CONCLUSION. In 8.9% of patients, TRO CT detected a significant noncoronary diagnosis that could explain acute chest pain, including pathologic findings that would not be identified on dedicated coronary CT angiography.
Diagnostic Yield of Triple-Rule-Out CT in an Emergency Setting Amelia M. Wnorowski, Ethan J. Halpern AJR 2016; 207:295–301 - “Acute coronary syndrome (ACS) accounts for a minority of acute chest pain presentations and was diagnosed in only 13% of patients who visited the emergency department for chest pain in 2007–2008 . However, ACS is a serious cause of chest pain, with an associated mortality rate of 3–33% and high associated morbidity, because up to 30% of patients with ACS who are discharged from the emergency department are rehospitalized within 6 months.”
Diagnostic Yield of Triple-Rule-Out CT in an Emergency Setting Wnorowski AM, Halpern EJ AJR 2016; 207:295–301 - “For the diagnosis of coronary artery disease, TRO CT has a sensitivity of 94.3%, a specificity of 97.4%, and a negative predictive value of 99%, findings that are similar to those obtained with the use of dedicated coronary CTA.”
Diagnostic Yield of Triple-Rule-Out CT in an Emergency Setting Wnorowski AM, Halpern EJ AJR 2016; 207:295–301 - “Although coronary disease was the most common diagnosis that explained chest pain, accounting for chest pain in 11.7% of our emergency department patients, TRO CT identified noncoronary diagnoses that could explain the presentation in 8.9% of our patient population. Pulmonary embolism was the most commonly noted noncoronary diagnosis.”
Diagnostic Yield of Triple-Rule-Out CT in an Emergency Setting Wnorowski AM, Halpern EJ AJR 2016; 207:295–301 - “On the basis of our retrospective review of CT findings, 30 (27.3%) of the patients with significant noncoronary diagnoses (28 of whom had pulmonary embolism and two of whom had an aortic pathologic finding) would not have been identified with the use of dedi- cated coronary CTA because of unopacified right-side circulation or limited z-axis cover- age (in patients with aortic pathologic find- ings).”
Diagnostic Yield of Triple-Rule-Out CT in an Emergency Setting Wnorowski AM, Halpern EJ AJR 2016; 207:295–301 - “In our patient population, more than 80% of patients had negative study results without significant coronary or noncoronary diagnoses. This is similar to the results of a previous study, in which 76% of patients did not require further testing. In the same study, TRO CT had a negative predictive value of 99.4% and was associated with no adverse outcomes.”
Diagnostic Yield of Triple-Rule-Out CT in an Emergency Setting Wnorowski AM, Halpern EJ AJR 2016; 207:295–301 - “Our experience with close to 1200 consecutive TRO CT studies over 10 years found that TRO CT identified significant and potentially fatal noncoronary diagnoses in 8.9% of the presenting population. The frequency of these noncoronary diagnoses is dependent on an appropriately selected patient population with a low to intermediate risk of ACS and for whom alternative diagnoses should also be considered, including pulmonary embolism and acute aortic pathology. TRO CT also identifies patients at risk for ACS and allows discharge of a majority of patients with negative study results.”
Diagnostic Yield of Triple-Rule-Out CT in an Emergency Setting Wnorowski AM, Halpern EJ AJR 2016; 207:295–301
- “Diagnosis and triage of ED patients with suspected acute coronary syndromes (ACS) consumes a large and increasing amount of health care resources. It has been estimated that more than 9 million ED patients with ACP are seen annually in the United States alone, with related health-care costs of $13 to $15 billion.”
SCCT guidelines on the use of coronary computed tomographic angiography for patients presenting with acute chest pain to the emergency department: A Report of the Society of Cardiovascular Computed Tomography Guidelines Committee Raff GL et al. Journal of Cardiovascular Computed Tomography 8 (2014) 254-271 - Diagnostic Options in the ER Setting for Chest Pain Patients
• exercise EKG treadmill testing,
• rest myocardial perfusion imaging (MPI),
• stress MPI
• stress echocardiography
• anatomic imaging by coronary CTA. - “ The accuracy of coronary CTA to predict an equal to or greater than 50% stenosis averaged to: 93% sensitivity, 79% specificity, 80% positive predictive value and 93% negative predictive value. These values compared favorably with rest-stress MPI, often considered the standard for noninvasive evaluation of ACP.”
SCCT guidelines on the use of coronary computed tomographic angiography for patients presenting with acute chest pain to the emergency department: A Report of the Society of Cardiovascular Computed Tomography Guidelines Committee Raff GL et al. Journal of Cardiovascular Computed Tomography 8 (2014) 254-271 - “Coronary CTA as compared with SOC resulted in a reduced median length of stay (8.6 hours vs 26.7 hours; P < .001), time to diagnosis (5.8 hours vs 21.0 hours; P < .001), and increase in direct discharges (47% vs 12%; P < .001). There were more major adverse cardiac events in the SOC vs the coronary CTA group within 30 days (6 events vs 2 events; P 1⁄4 .18), but this difference was not significant. ROMICAT-II also reported costs of care including hospital costs, which were similar between CTA and SOC ($4026 vs $3874).”
SCCT guidelines on the use of coronary computed tomographic angiography for patients presenting with acute chest pain to the emergency department: A Report of the Society of Cardiovascular Computed Tomography Guidelines Committee Raff GL et al. Journal of Cardiovascular Computed Tomography 8 (2014) 254-271 - “The ROMICAT-II trial randomized 1000 patients to either early coronary CTA or to SOC. Notable differences to the prior randomized studies were that TIMI scores did not limit entry criteria and that the SOC included any available management strategy deemed appropriate by the treating physicians. These choices included EKG treadmill testing, stress echo and stress single- photon emission CT.”
SCCT guidelines on the use of coronary computed tomographic angiography for patients presenting with acute chest pain to the emergency department: A Report of the Society of Cardiovascular Computed Tomography Guidelines Committee Raff GL et al. Journal of Cardiovascular Computed Tomography 8 (2014) 254-271 - “A quality assurance program is recommended, with quality targets including: a diagnostic-quality scan rate of !95%, a quarterly median radiation dose rate within the reference level (currently, 12 mSv, based on the most recent guideline) established by the SCCT guidelines on radiation dose and dose-optimization strategies in cardiovascular CT, and a quarterly comparative review of cases with both coronary CTA and invasive angiography that demonstrates a median accuracy of at least 75% per-patient accuracy.”
SCCT guidelines on the use of coronary computed tomographic angiography for patients presenting with acute chest pain to the emergency department: A Report of the Society of Cardiovascular Computed Tomography Guidelines Committee Raff GL et al. Journal of Cardiovascular Computed Tomography 8 (2014) 254-271 - Cardiac CT in the ER: Indications
Acute chest pain patients with clinically suspected coronary ischemia
• EKG negative or indeterminate for myocardial ischemia
• Low-intermediate pretest likelihood by risk stratification tools, for example, TIMI 0-2 risk score (low) or 3-4 (intermediate) risk
• Equivocal or inadequate previous functional testing during index ED or within previous 6 months - Factors Leading to Poor Quality Cardiac CTA
• Heart rate > site maximum for reliably diagnostic scans after beta blockers
• Contraindications to beta blockers and inadequate HR control
• Atrial fibrillation or other markedly irregular rhythm
• BMI >39 kg/m2 - Absolute Contraindications for Cardiac CT
• Acute coronary syndromes
• GFR <30 unless on chronic dialysis, or evidence of ATN
• Previous anaphylaxis after iodinated contrast administration
• Previous episode of contrast allergy after adequate steroid/antihistamine preparation Inability to cooperate, including inability to raise arms
• Pregnancy or uncertain pregnancy status in premenopausal women - Prospective vs Retrospective Cardiac CT Scanning
• Retrospectively gated helical scanning
• Use in patients with heart rates higher than prospective-triggered target range or significantly irregular rhythm
• Acquisition window width
Heart rate <65 beats/min: 65%-75%
Heart rate 66-72 beats/min: 60%-80%
Heart rate >72 beats/min: 35%-80% - Prospective vs Retrospective Cardiac CT Scanning
• Prospectively gated helical scanning
• Use in patients with stable sinus rhythm below the target heart rate (typically 65 beats/min) - Triage Patterns for CCTA in the Eergency Room
- “Use of advanced scanners facilitating prospectively triggered or high-pitch spiral scan modes results in marked dose reduction across a variety of cardiovascular studies, with no compromise in image quality.”
CT dose reduction using prospectively triggered or fast-pitch spiral technique employed in cardiothoracic imaging (the CT dose study) Chinnaiyan KM et al. J Cardiovascular Comput Tomogr 8 (2014) 205-214 - “The second-generation, 128-slice, dual-source CT uses a pitch value of 3.2 in the high-pitch, spiral scan mode, in which prospective ECG-triggered spiral data acquisition is completed within a single cardiac cycle for sufficiently short scan ranges and sufficiently long R-R intervals. In this mode, the entire heart is covered in approximately 260 ms and the chest in 700 ms. The second detector array is used to fill in the sam- pling gaps, and cross-sectional images are reconstructed from the acquired data with a temporal resolution of 75 ms, with an offset of approximately 0.65 ms.”
CT dose reduction using prospectively triggered or fast-pitch spiral technique employed in cardiothoracic imaging (the CT dose study) Chinnaiyan KM et al. J Cardiovascular Comput Tomogr 8 (2014) 205-214

- “TRO was associated with slightly higher yield of PE and AD, specifically in the emergency department. This benefit comes with higher nondiagnostic image quality, radiation, and contrast doses. Although TRO may be of value in selected patients, its indiscriminate use is not warranted. The appropriate use of TRO needs to be further defined.” Triple Rule Out Versus Coronary CT Angiography in Patients With Acute Chest Pain : Results From the ACIC Consortium Alfred C. Burris II et al. JACC Cardiovasc Imaging. 2015 Jul;8(7):817-25
- “TRO had higher median radiation (9.1 mSv vs. 6.2 mSv; p < 0.0001) and mean contrast (113 ± 6 ml vs. 89 ± 17 ml; p < 0.0001) doses. Nondiagnostic images were frequent in TRO (9.4% vs. 6.5%; p < 0.0001).” Triple Rule Out Versus Coronary CT Angiography in Patients With Acute Chest Pain : Results From the ACIC Consortium Alfred C. Burris II et al. JACC Cardiovasc Imaging. 2015 Jul;8(7):817-25
- “It is important to note that even though the rates of PE and AD on coronary CTA (with limited field of view) were lower than in dedicated protocols, they were high for unsuspected but clinically important diagnoses. However, >97% of TRO studies showed neither AD nor PE. These discordant findings between scan intention and results highlight the fact that the diagnosis of acute chest pain can be challenging, particularly because clinical presentations are often atypical or unclear.” Triple Rule Out Versus Coronary CT Angiography in Patients With Acute Chest Pain : Results From the ACIC Consortium Alfred C. Burris II et al. JACC Cardiovasc Imaging. 2015 Jul;8(7):817-25
- “TRO was associated with a 45% higher frequency of nondiagnostic image quality compared with coronary CTA. Although the TRO scan type itself was not a significant predictor of nondiagnostic image quality on multivariate analysis, it is likely that this protocol is affected by the type of contrast bolus used as well as body habitus. Higher heart rates and ectopy (resulting in motion artifacts) and clinical conditions that may result in the patient’s inability to lie flat were found to be significant predictive factors for scan uninterpretability.” Triple Rule Out Versus Coronary CT Angiography in Patients With Acute Chest Pain : Results From the ACIC Consortium Alfred C. Burris II et al. JACC Cardiovasc Imaging. 2015 Jul;8(7):817-25
- “TRO may be considered when clinical features and initial laboratory data (e.g., indeterminate troponin and elevated d-dimer) raise concern for: 1) obstructive CAD; and 2) PE or AD. Therefore, we propose an algorithm that divides patients presenting with acute symptoms into 3 risk groups: high, low to intermediate, and very low (noncardiac) .” Triple Rule Out Versus Coronary CT Angiography in Patients With Acute Chest Pain : Results From the ACIC Consortium Alfred C. Burris II et al. JACC Cardiovasc Imaging. 2015 Jul;8(7):817-25
- “In this large registry, TRO was associated with slightly higher diagnostic yield for PE and AD compared with coronary CTA, particularly in the ED, and was used more often in younger women. Additionally, TRO is associated with significantly higher radiation and contrast doses compared with coronary CTA. Thus, although feasible, clinical criteria for TRO use and appropriateness must be further defined.” Triple Rule Out Versus Coronary CT Angiography in Patients With Acute Chest Pain : Results From the ACIC Consortium Alfred C. Burris II et al. JACC Cardiovasc Imaging. 2015 Jul;8(7):817-25
- “In this large registry, TRO was associated with slightly higher diagnostic yield for PE and AD compared with coronary CTA, particularly in the ED, and was used more often in younger women. Additionally, TRO is associated with significantly higher radiation and contrast doses compared with coronary CTA. Thus, although feasible, clinical criteria for TRO use and appropriateness must be further defined.” Triple Rule Out Versus Coronary CT Angiography in Patients With Acute Chest Pain : Results From the ACIC Consortium Alfred C. Burris II et al. JACC Cardiovasc Imaging. 2015 Jul;8(7):817-25

- Can you do a triple rule out (TRO)-
- Answer: yes you can
- Real Question is whether you should you be doing triple rule out studies in the ER - OBJECTIVES:The objective was to compare the image quality, diagnostic accuracy, radiation exposure, and contrast volume of "triple rule-out" (TRO) computed tomography (CT) to other diagnostic modalities commonly used to evaluate patients with nontraumatic chest pain (dedicated coronary, pulmonary embolism [PE], and aortic dissection CT; invasive coronary angiography; and nuclear stress testing).
Triple rule-out computed tomographic angiography for chest pain: a diagnostic systematic review and meta-analysis
Ayaram D et al.
Acad Emerg Med 2013 Sep: 20(9);861-71 - “Eleven studies enrolling 3,539 patients (791 TRO and 2,748 non-TRO) were included (one randomized controlled trial and 10 observational). There was no significant difference in image quality between TRO and dedicated CT scans. TRO CT had the following pooled diagnostic accuracy estimates for coronary artery disease: sensitivity of 94.3% (95% confidence interval [CI] = 89.1% to 97.5%), specificity of 97.4% (95% CI = 96.1% to 98.4%), positive likelihood ratio (LR+) of 17.71 (95% CI = 3.92 to 79.96), and negative likelihood ratio (LR-) of 0.08 (95% CI = 0.02 to 0.27).”
Triple rule-out computed tomographic angiography for chest pain: a diagnostic systematic review and meta-analysis
Ayaram D et al.
Acad Emerg Med 2013 Sep: 20(9);861-71 - “There were insufficient numbers of patients with PE or aortic dissection to generate diagnostic accuracy estimates for these conditions. Use of TRO CT involved greater radiation exposure (mean difference [MD] = 4.84 mSv, 95% CI = 1.65 to 8.04 mSv) and contrast exposure (MD = 38.0 mL, 95% CI = 28.1 to 48.0 mL) compared to non-TRO CT patients.”
- Triple rule-out computed tomographic angiography for chest pain: a diagnostic systematic review and meta-analysis
Ayaram D et al.
Acad Emerg Med 2013 Sep: 20(9);861-71 - “Triple rule-out computed tomography is highly accurate for detecting coronary artery disease. Given the low (<1%) prevalence of pulmonary embolism and aortic dissection in the included studies, and the increased radiation and contrast exposure, there are insufficient data to recommend use of triple rule-out computed tomography in the diagnosis of these conditions.”
Triple rule-out computed tomographic angiography for chest pain: a diagnostic systematic review and meta-analysis
Ayaram D et al.
Acad Emerg Med 2013 Sep: 20(9);861-71 - CONCLUSIONS:
“Triple rule-out CT is highly accurate for detecting coronary artery disease. Given the low (<1%) prevalence of PE and aortic dissection in the included studies, and the increased radiation and contrast exposure, there are insufficient data to recommend use of TRO CT in the diagnosis of these conditions.”
Triple rule-out computed tomographic angiography for chest pain: a diagnostic systematic review and meta-analysis
Ayaram D et al.
Acad Emerg Med 2013 Sep: 20(9);861-71 - “ Herein, we provide a 10-step approach for establishing a successful coronary CT angiography program in the emergency department. The importance of strategic planning and multidisciplinary collaboration is emphasized. Patient selection and preparation guidelines for coronary CT angiography are reviewed with straightforward protocols that can be adapted and modified to clinical sites, depending on available cardiac imaging capabilities. Technical parameters and patient-specific modifications are also highlighted to maximize the likelihood of diagnostic quality examinations. Practical suggestions for quality control, process monitoring, and standardized reporting are reviewed. Finally, the role of a "triple rule-out" protocol is featured in the context of acute chest pain evaluation in the emergency department.”
Establishing a successful coronary CT angiography program in the emergency department:official writing of the Fellow and Resident Leaders of the Society of Cardiovascular Computed Tomography (FIRST)
Maroules CD, Blaha MJ, El-Haddad MA, Cury RC
J Cardiovasc Comput Tomogr 2013 May-Jun; 7(3):150-6 - “ Herein, we provide a 10-step approach for establishing a successful coronary CT angiography program in the emergency department. The importance of strategic planning and multidisciplinary collaboration is emphasized. ..Finally, the role of a "triple rule-out" protocol is featured in the context of acute chest pain evaluation in the emergency department.”
Establishing a successful coronary CT angiography program in the emergency department:official writing of the Fellow and Resident Leaders of the Society of Cardiovascular Computed Tomography (FIRST)
Maroules CD, Blaha MJ, El-Haddad MA, Cury RC
J Cardiovasc Comput Tomogr 2013 May-Jun; 7(3):150-6 - “ Current data show that in intermediate or low risk patients this method is suitable to reliably rule out coronary heart disease. In addition, attention is paid to the major differential diagnoses of acute coronary syndrome,
particularly pulmonary embolism and aortic dissection. Here the diagnostic method of choice is thoracic CT, possibly also in combination with CCTA aiming at a triple rule-out.”
Clinical assessment of chest pain and guidelines for imaging
J. Gruettner et al.
European Journal of Radiology 81 (2012) 3663– 3668 
Clinical assessment of chest pain and guidelines for imaging J. Gruettner et al. European Journal of Radiology 81 (2012) 3663– 3668- “Here the classic sequence of basic cardiac diagnostics including case history (cardiac risk factors), physical examination (haemodynamic and respiratory vital parameters), ECG (ST segment analysis) and laboratory risk markers (troponin levels) is paramount. The focus is, on the one hand, on timely indication for percutaneous catheterization, especially in patients at high cardiac risk with or without ST-segment elevation in the ECG, and, on the other hand, on the possibility of safely discharging patients with intermediate or low cardiacrisk after non-invasive exclusion of a coronary syndrome.”
Clinical assessment of chest pain and guidelines for imaging
J. Gruettner et al.
European Journal of Radiology 81 (2012) 3663– 3668 
Clinical assessment of chest pain and guidelines for imaging
J. Gruettner et al.
European Journal of Radiology 81 (2012) 3663– 3668- “Aim of this study was to retrospectively compare the image quality and the radiation dose of an ultra high pitch CT scan for the evaluation of pulmonary embolism and visualization of cardiac
structures in comparison to our institution’s standard pulmonary embolism protocol.”
Clinical utility of ultra high pitch dual source thoracic CT imaging ofacute pulmonary embolism in the emergency department: Are weone step closer towards a non-gated triple rule out-
Hou DJ et al.
European Journal of Radiology 82 (2013) 1793–1798 - “For the ultra high pitch protocol, 14% (8/57) were positive for pulmonary embolus compared to
13.7% (8/58) for the standard pitch group. 98.2% of the ultra high pitch scans were diagnostic for pulmonary embolus vs. 94.8% of the standard protocol. Visualization of cardiac structures was significantly improved with the ultra high pitch protocol (p < 0.0001). Significantly more lung parenchymal motion was observed on the standard protocol (p < 0.0001). The mean pulmonary vessel attenuation, SNR, and CNR were not significantly different. The mean effective dose was lower for the ultra high pitch studies (4.09 mSv ±0.78 vs. 7.72 mSv ±2.60, p < 0.0001).
Clinical utility of ultra high pitch dual source thoracic CT imaging ofacute pulmonary embolism in the emergency department: Are weone step closer towards a non-gated triple rule out-
Hou DJ et al.
European Journal of Radiology 82 (2013) 1793–1798 - “ Conclusion: Ultra high pitch CT imaging for pulmonary embolus is a technique which has potential to
assess motion free evaluation of most cardiac structures and proximal coronary arteries at lower radiation
doses.”
Clinical utility of ultra high pitch dual source thoracic CT imaging ofacute pulmonary embolism in the emergency department: Are weone step closer towards a non-gated triple rule out-
Hou DJ et al.
European Journal of Radiology 82 (2013) 1793–1798 - “This test exposes patients to a much higher dose of radiation than standard CT coronary angiography. Even with the latest technology and prospective gating the mean radiation dose isreported to be 7.5-16 mSv. Furthermore, both pulmonary embolism and aortic dissection are rare. In one large series of more than 2000 CT scans no diagnoses of aortic dissection were made, and in those presenting to an emergency department with acute chest pain, pulmonary embolism and dissection combined amounted to only 0.2% of diagnoses.”
CT triple rule-out examination: higher radiation dose
without clinical benefit
Ripley DP et al.
BMJ 2013;347:f5118 - “CT coronary angiography can be used to support early dischargein people presenting with acute chest pain and is established in National Institute for Health and Care Excellence guidance for the investigation of those with a low pre-test likelihood for coronary artery disease. The triple rule-out CT examination results in high exposure to ionizing radiation with no confirmed clinical benefit. Advanced imaging techniques should be used to support clinical decision making, not instead of it. To paraphrase the BMJ series by Spence, perhaps this is a case of “Bad Medicine” rather than Too Much Medicine..”
CT triple rule-out examination: higher radiation dose
without clinical benefit
Ripley DP et al.
BMJ 2013;347:f5118 - “Conclusion: Coronary CTA and TRO-CTA allow a rapid and safe discharge in the majority of patients presenting with acute chest pain and an intermediate risk for ACS while at the same time identifies those with significant coronary artery stenosis.”
Coronary computed tomography and triple rule out CT in patients with acute chest pain and an intermediate cardiac risk profile. Part 1: Impact on patient management
Gruettner J etal.
European Journal of Radiology 82 (2013) 100– 105 
Coronary computed tomography and triple rule out CT in patients with acute chest pain and an intermediate cardiac risk profile. Part 1: Impact on patient management
Gruettner J etal.
European Journal of Radiology 82 (2013) 100– 105- “In conclusion, our study demonstrates that coronary CTA and TRO-CTA both can accurately rule out ACS in the majority of patients with acute chest pain and an intermediate cardiac risk profile and identify those with significant coronary artery stenosis. Given the large number of patients with acute chest pain andan intermediate cardiac risk profile, early coronary coronary CTA or TRO-CTA may significantly improve patient management in emergency departments. In addition, anatomic imaging of the whole chest with TRO-CTA can help to detect non-coronary causes of acute chest pain and thus helping emergency department physicians to rapidly direct patients.”
Coronary computed tomography and triple rule out CT in patients with acute chest pain and an intermediate cardiac risk profile. Part 1: Impact on patient management
Gruettner J etal.
European Journal of Radiology 82 (2013) 100– 105 - Objective: To evaluate the economic impact of integrating coronary CT angiography (cCTA) or whole chest
“triple-rule-out” CTA (TRO-CTA) in the work-up of patients with acute chest pain. - Conclusion: Integrating cCTA or TRO-CTA in a SOC algorithm can safely reduce the number of hospitalized
patients and reduce total health care costs.
Coronary computed tomography and triple rule out CT in patients with acute
chest pain and an intermediate cardiac risk for acute coronary syndrome Part 2: Economic aspects
Henzler T et al.
European Journal of Radiology 82 (2013) 106– 111 - “In conclusion, integrating cCTA in a SOC algorithm for the workup of patients with acute chest pain and an intermediate risk for ACS can reduce the number of hospitalized patients while at the same time reduce overall health care costs.”
Coronary computed tomography and triple rule out CT in patients with acute
chest pain and an intermediate cardiac risk for acute coronary syndrome Part 2: Economic aspects
Henzler T et al.
European Journal of Radiology 82 (2013) 106– 111 
Coronary computed tomography and triple rule out CT in patients with acute
chest pain and an intermediate cardiac risk for acute coronary syndrome Part 2: Economic aspects
Henzler T et al.
European Journal of Radiology 82 (2013) 106– 111- “ A TRO protocol may be considered if an additional suspicion of pulmonary embolism or acute aortic disease is present,
when using a CT with 64-slices or more. Radiation and contrast exposure needs to be balanced and outweighed
with risks and benefits when using 64-slice CT, and low-radiation dose CT scan techniques applied whenever possible.”
Cardiac CT in the emergency department:
Convincing evidence, but cautious
implementation
Cury RC et al.
J Nucl Cardiol 2011;18:331–41. - “ It appears that much of the decision on ordering or nor ordering a TRO or coronary CT will be for the moment guided and perhaps limited by non-research-based factors: technical availability to obtain and interpret images, hospital willingness to provide this imaging, and patient willingness to pay for it.”
Triple rule out: why it is not ready to roll out.
Acad Emerg Med. 2013 Sep;20(9):934-6. - Courtney DM
(commentary)
“ It is unlikely that the future of cost containment at both the CMS/third party insurer level or the hospital/accountable care organization level will support an expanding role of TRO without additional evidence that it improves disease detection and preserves health in some quantifiable way.”
Triple rule out: why it is not ready to roll out.
Acad Emerg Med. 2013 Sep;20(9):934-6.
Courtney DM
(commentary)
- “ In 2007, there were about 117 million visits to the emergency department (ED) in the United States. Approximately 8 million of these patients—the second largest cohort—presented with chest pain. Generally 15% to 30% of patients who present to the ED with nontraumatic chest pain have acute coronary syndrome (ACS).”
Coronary and Cardiac Computed Tomography in the Emergency Room: Current Status and Future Directions
Cook TS et al.
J Thorac Imaging 2013;28:204-216 - “ CCTA has now been validated using several large multicenter trials that demonstrate its safety and efficiency. However, concerns remain about increased resource utilization and radiation exposure, and the role of new biomarkers may change how we practice. Specifically, patients with negative ultrahigh-sensitivity troponins may not require imaging; however, these new biomarkers are rarely unequivocally negative.”
Coronary and Cardiac Computed Tomography in the Emergency Room: Current Status and Future Directions
Cook TS et al.
J Thorac Imaging 2013;28:204-216
- “ Chest pain patients with negative or mild nonobstructive CTA findings can be safely discharged from the ED without further testing. Implementation of a dedicated chest pain triage protocol is critical for the success of a coronary CTA program.”
Triage of Patients Presenting With Chest Pain to the Emergency Department: Implementation of Coronary CT Angiography in a Large Urban Health Care System
Cury RC et al.
AJR 2013;200:57-65 - What patient went for CTA-
- Low to intermediate risk of acute coronary syndrome (TIMI (thrombolysis in myocardial infarction) risk score <2)
- Typical angina < 30 minutes, normal ECG findings
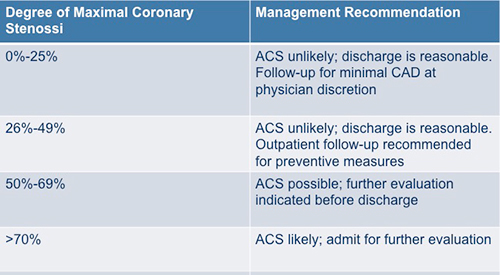
- Atypical symptoms, normal or nondiagnostic ECG findings, negative cardiac enzyme results - CTA Triage: 4 Groups
0 Low (negative CT findings) 1 Mid (1-49% stenosis) 2 Moderate (50-69% stenosis) 3 Severe (greater than or equal to 70% stenosis) - “ The sensitivity of CTA was 94%.The rate of MACEs in patients with stenosis of greater than 70% or greater (8.3%) was significantly higher than in patients with negative CTA findings(0%)or those with mild stenosis (0.2%). A 51% decrease in LOS-from 28.8 to 14.4 hours-was noted after implementation of the dedicated chest pain protocol.”
Triage of Patients Presenting With Chest Pain to the Emergency Department: Implementation of Coronary CT Angiography in a Large Urban Health Care System
Cury RC et al.
AJR 2013;200:57-65 - “Although fewer than 5% of patients with acute chest pain present with ST-segment elevation myocardial infarction (STEMI) and are directly transferred to the catheterization laboratory, the majority of patients require admission to an ED center unit for further diagnostic workup.”
Triage of Patients Presenting With Chest Pain to the Emergency Department: Implementation of Coronary CT Angiography in a Large Urban Health Care System
Cury RC et al.
AJR 2013;200:57-65 - “Coronary CTA and TRO-CTA allow a rapid and safe discharge in the majority of patients presenting with acute chest pain and an intermediate risk for ACS while at the same time identifies those with significant coronary artery stenosis.”
Coronary computed tomography and triple rule out CT in patients with acute chest pain and an intermediate cardiac risk profile. Part 1: Impact on patient management.
Gruettner J et al.
Eur J Radiol 2013 Jan; 82(1):100-5 - “Based on a negative coronary CTA 60 of 100 patients were discharged on the same day. None of the discharged patients showed MACE during the 90-day follow-up. Coronary CTA revealed a coronary stenosis >50% in 19 of 100 patients. ICC confirmed significant coronary stenosis in 17/19 patients. Among the 17 true positive patients, 9 underwent percutaneous coronary intervention with stent implantation, 7 were received intensified medical therapy, and 1 patient underwent coronary artery bypass surgery.”
Coronary computed tomography and triple rule out CT in patients with acute chest pain and an intermediate cardiac risk profile. Part 1: Impact on patient management.
Gruettner J et al.
Eur J Radiol 2013 Jan; 82(1):100-5 - “A TRO-CTA protocol was performed in 36/100 patients due to elevated d-dimer levels. Pulmonary embolism was present in 5 patients, pleural effusion of unknown etiology in 3 patients, severe right ventricular dysfunction with pericardial effusion in 1 patient, and an incidental bronchial carcinoma was diagnosed in 1 patient.”
Coronary computed tomography and triple rule out CT in patients with acute chest pain and an intermediate cardiac risk profile. Part 1: Impact on patient management.
Gruettner J et al.
Eur J Radiol 2013 Jan; 82(1):100-5 - “Due to the advances of multi-detector CT technology, dedicated coronary CT angiography provides the potential to rapidly and reliably diagnose or exclude acute coronary artery disease. Life-threatening causes of chest pain, such as aortic dissection and pulmonary embolism can simultaneously be assessed with a single scan, sometimes referred to as "triple rule out" scan. With appropriate patient selection, cardiac CT can accurately diagnose heart disease or other sources of chest pain, markedly decrease health care costs, and reliably predict clinical outcomes.”
Cardiac CT for the assessment of chest pain: imaging techniques and clinical results
Becker HC, Johnson T
Eur J Radiol Dec;81(12):3675-9
- “ MDCT with virtual angioscopy can depict the configuration of intimal tears in cases of thoracic aortic dissection, which may facilitate therapeutic planning.”
Intimal Tears in Thoracic Aortic Dissection: Appearance on MDCT With Virtual Angioscopy
Maldjiian PD eta l.
AJR 2012; 198:955-961 - “MDCT can depict feature helping to differentiate the true lumen from the false lumen. The false lumen is usually larger than the true lumen and commonly deforms the shape of the true lumen.”
Intimal Tears in Thoracic Aortic Dissection: Appearance on MDCT With Virtual Angioscopy
Maldjiian PD eta l.
AJR 2012; 198:955-961 - “Flow in the false lumen is usually slower than that in the true lumen; hence the attenuation of the false lumen tends to be lower and more heterogeneous than the attenuation of the true lumen because of mixing of contrast agent with unopacified blood.”
Intimal Tears in Thoracic Aortic Dissection: Appearance on MDCT With Virtual Angioscopy
Maldjiian PD eta l.
AJR 2012; 198:955-961
- “Comprehensive cardiothoracic CT scanning was feasible, with a similar diagnostic yield to dedicated protocols. However, it did not reduce the length of stay, rate of subsequent testing, or costs. In conclusion, although this "triple rule out" protocol might be helpful in the evaluation of select patients, these findings suggest that it should not be used routinely with the expectation that it will improve efficiency or reduce resource use.”
Usefulness of comprehensive cardiothoracic computed tomography in the evaluation of acute undifferentiated chest discomfort in the emergency department (CAPTURE)
Rogers IS et al.
Am J Cardiol 2011 March 1;107(5):643-650 - “We conducted a randomized diagnostic trial to compare the efficiency of a comprehensive cardiothoracic CT examination in the evaluation of patients presenting to the emergency department with undifferentiated acute chest discomfort or dyspnea. We randomized the emergency department patients clinically scheduled to undergo a dedicated CT protocol to assess coronary artery disease, pulmonary embolism, or aortic dissection to either the planned dedicated CT protocol or a comprehensive cardiothoracic CT protocol..”
Usefulness of comprehensive cardiothoracic computed tomography in the evaluation of acute undifferentiated chest discomfort in the emergency department (CAPTURE)
Rogers IS et al.
Am J Cardiol 2011 March 1;107(5):643-650 - "The image quality of triple rule out CTA is comparable to that of dedicated coronary CTA, showing no statistically significant difference in motion artifacts or opacification, and therefore may be alternative and useful diagnostic study in a select group of emergency patients."
Triple Rule-out and Dedicated Coronary Artery CTA: Comparison of Coronary Image Quality
Rahmani N, Jeudy J, White CS
Acad Radiol 2009; 16:604-609 - “ Therefore, in ED patients who have a low clinical suspicion of pulmonary embolism and acute aortic syndrome, especially younger patients, dedicated coronary CT angiography accompanied by modifications to reduce radiation dose is recommended.”
Coronary CT angiography in emergency department patients with acute chest pain: triple rule-out protocol versus dedicated coronary CT angiography
Lee Hy, Yoo SM, White CS
Int J Cardiovasc Imaging 2009 Mar;25(3):319-26 - “ In ED patients with atypical chest pain and low to intermediate risk, the triple rule-out protocol may be preferred, especially in older patients who have relatively lower risk of lifelong radiation-induced cancer. However, the increased radiation dose resulting from the extended volume coverage with this protocol should be fully considered prior to performing this protocol.”
Coronary CT angiography in emergency department patients with acute chest pain: triple rule-out protocol versus dedicated coronary CT angiography
Lee Hy, Yoo SM, White CS
Int J Cardiovasc Imaging 2009 Mar;25(3):319-26 - “ In ED patients with atypical chest pain and low to intermediate risk, the triple rule-out protocol may be preferred, especially in older patients who have relatively lower risk of lifelong radiation-induced cancer. However, the increased radiation dose resulting from the extended volume coverage with this protocol should be fully considered prior to performing this protocol. Therefore, in ED patients who have a low clinical suspicion of pulmonary embolism and acute aortic syndrome, especially younger patients, dedicated coronary CT angiography accompanied by modifications to reduce radiation dose is recommended.”
Coronary CT angiography in emergency department patients with acute chest pain: triple rule-out protocol versus dedicated coronary CT angiography
Lee Hy, Yoo SM, White CS
Int J Cardiovasc Imaging 2009 Mar;25(3):319-26 - “Consecutive cCTA examinations performed by a single radiologist over 1 year were reviewed. Biphasic injection protocols were employed: 70 mL of optiray-350 followed by 40 mL of saline injected at 5.5 mL/second for dedicated cCTA; 70 mL of optiray-350 followed by 25 mL of the contrast diluted with 25 mL of saline injected at 5.0 mL/second for TRO-CTA. Two independent cardiovascular radiologists reviewed the coronary vessels in each case and rated diagnostic image quality on a 5 point scale (1, suboptimal; 3, adequate; 5, excellent). Vascular enhancement was measured in the coronary arteries, aorta, and pulmonary arteries.”
Comparison of Image Quality and Arterial Enhancement with a Dedicated Coronary CTA Protocol versus a Triple Rule-Out Coronary CTA Protocol
Halpern EJ et al.
Acad Radiol 2009 Sep;16(9):1039-1048 - “There was excellent interobserver agreement between the cardiovascular radiologists (kappa = 0.91). Coronary image quality score were similar among 260 dedicated cCTA studies and 168 TRO-CTA studies (mean: 3.8-3.9. P > .18). At least one coronary segment demonstrated suboptimal image quality in 8% of examinations, including 18 dedicated cCTA studies and 16 TRO studies (P = .94). Enhancement was greater in the distal thoracic aorta of TRO patients (336 vs. 311 Hounsfield units; P = .01); no other significant differences in enhancement were identified in the aorta and coronary arteries of dedicated cCTA and TRO studies. Vascular enhancement was adequate for diagnostic evaluation of the pulmonary arteries in all TRO studies.”
Comparison of Image Quality and Arterial Enhancement with a Dedicated Coronary CTA Protocol versus a Triple Rule-Out Coronary CTA Protocol
Halpern EJ et al.
Acad Radiol 2009 Sep;16(9):1039-1048 - “Rational and Objectives
To compare the image quality of dedicated coronary computed tomography angiography (cCTA) to that of triple rule-out (TRO) CTA designed to evaluate the coronary arteries, thoracic aorta, and pulmonary arteries.
Conclusions
A TRO-CTA protocol using 95 mL of contrast can provide comparable coronary image quality and coronary vascular enhancement as compared to dedicated cCTA with 70 mL of contrast.
Comparison of Image Quality and Arterial Enhancement with a Dedicated Coronary CTA Protocol versus a Triple Rule-Out Coronary CTA Protocol
Halpern EJ et al.
Acad Radiol 2009 Sep;16(9):1039-1048 - Triple Rule Out: Challenges
-Fast Flash acquisition with high pitch values (3.2 or greater) is ideal to minimize contrast volume used by decreasing scan times to 1-2 seconds
-Split bolus common with second bolus usually having lower injection rates (5 cc vs 3 cc) and volumes (80-100 cc vs 20-30 cc). Split injection with second bolus of 70%-30% (contrast/saline) for longer injection volumes and increased volume injection times - Triple Rule Out Challenges
-Optimal opacification of both the pulmonary artery and the aortic circulations must be optimally opacified
-Although both peaks occur in close proximity the pulmonary arteries opacify well 10-12 seconds before the aorta
-To maintain optimal opacification you can increase contrast volume (130 cc) or decrease injection rates to lenghen the transit opacification time (4 cc vs 5-6cc/sec) - Triple Rule Out Protocols:
-You need to perform 2 or 3 quality exams in one CT acquisition
-Coronary CTA
-Aortic Evaluation for Dissection or Aneurysm
-Pulmonary arteriograms - “ A triple rule out protocol (TRO) may be considered if an additional suspicion of pulmonary embolism or acute aortic disease is present, when using 64-slices or more.”
Cardiac CT in the emergency department: Convincing evidence, but cautious implementation
Cury RC ey al
J Nucl Cardiol 2011;18:331-341 - “ The focus of this article is to review the current literature of the uses of Coronary CTA and “triple rule out” protocols in the emergency department setting and to provide a chest pain algorithm, showing how Coronary CTA can be implemented effectively in clinical focus.”
Cardiac CT in the emergency department: Convincing evidence, but cautious implementation
Cury RC ey al
J Nucl Cardiol 2011;18:331-341 - “ The focus of this article is to review the current available data in Coronary CTA and the extended Coronary CTA protocol or the so-called triple rule out scans in patients presenting to the ED with chest pain.”
Cardiac CT in the emergency department: Convincing evidence, but cautious implementation
Cury RC et al
J Nucl Cardiol 2011;18:331-341 - “Continued technical improvements in acquisition speed and spatial resolution of computed tomography images, and development of more efficient image reconstruction algorithms which reduce patient exposure to radiation and contrast, may result in increased popularity of MDCT for "triple rule-out”.
Evaluation of Acute Chest Pain in the Emergency Department: “Triple Rule-Out” Computed Tomography Angiography
Yoon ES, Wann S
Cardiol Rev 2011 May-Jun;19(3):115-21 - “ The triple rule-out protocol is most appropriate for patients who present with acute chest pain, but are judged to have low to intermediate increased risk for acute coronary syndrome, and whose chest pain symptoms might also be attributed to acute pathologic conditions of the aorta or pulmonary arteries. MDCT should not be used as a routine screening procedure.”
Evaluation of Acute Chest Pain in the Emergency Department: “Triple Rule-Out” Computed Tomography Angiography
Yoon ES, Wann S
Cardiol Rev 2011 May-Jun;19(3):115-21 - “MDCT is used for the detection of 3 of the most common life-threatening causes of chest pain-coronary artery disease, acute aortic syndrome, and pulmonary emboli. While triple rule-out protocol can be very useful and potentially cost effective when used appropriately, concern has risen regarding the overuse of this technology, which could expose patients to unnecessary radiation and iodinated contrast.”
Evaluation of Acute Chest Pain in the Emergency Department: “Triple Rule-Out” Computed Tomography Angiography
Yoon ES, Wann S
Cardiol Rev 2011 May-Jun;19(3):115-21 - What is a triple rule-out CT scan?
-Coronary artery stenosis >50%
-Aortic dissection
-Pulmonary embolism - “ Compared with cardiac CT, the triple rule out approach was associated with higher radiation dose (12.0±5.6 mSv versus 8.2±4.0 mSv), a greater incidence of subsequent emergency center evaluations, and more downstream pulmonary embolism protocol CT angiography.”
Comparative diagnostic yield and 3 month outcomes of “triple rule-out” and standard protocol coronary CT angiography in the evaluation of acute chest pain
Madder RD et al.
J Cardiovascular Comput Tomogr (2011)5, 165-171 - “ Among patients with acute chest pain, a triple rule-out approach resulted in higher radiation exposure compared with cardiac CT, but was not associated with improved diagnostic yield, reduced clinical events, or diminished downstream resource use.”
Comparative diagnostic yield and 3 month outcomes of “triple rule-out” and standard protocol coronary CT angiography in the evaluation of acute chest pain
Madder RD et al.
J Cardiovascular Comput Tomogr (2011)5, 165-171 - “ Among 2068 patients (272 triple rule-out and 1796 cardiac CT angiograms) the composite diagnostic yield was 14.3% with triple rule-out and 16.3% with cardiac CT and was driven by the diagnosis of obstructive pulmonary disease.”
Comparative diagnostic yield and 3 month outcomes of “triple rule-out” and standard protocol coronary CT angiography in the evaluation of acute chest pain
Madder RD et al.
J Cardiovascular Comput Tomogr (2011)5, 165-171 "Currently available evidence suggests that CT-based approaches with modern scan technology are safe, accurate, and potentially cost-saving, although large scale clinical trials are needed to ascertain the precise role of CT in the evaluation of chest pain."
Cardiac CT in the Assessment of Acute Chest Pain in the Emergency Department
Bastarrika G et al.
AJR 2009; 193:397-409"Three important life threatening causes of chest pain are aortic dissection, pulmonary embolism, and acute coronary syndrome. Simple clinical tools should be applied to exclude these diagnoses and avoid CT whenever possible."
Role of computed tomography in the evaluation of acute chest pain
Urbania TH et al.
J Cardiovasc Comput Tomogr (2009) 3. Supplement 1, S13-S22"Triple rule out” protocols designed to simultaneously assess the aorta, pulmonary arteries and coronary arteries are a comprimise between dedicated protocols for each diagnosis. The diagnostic value and appropriate clinical use of these protocols remain to be shown by randomized, controlled, outcomes based trials."
Role of computed tomography in the evaluation of acute chest pain
Urbania TH et al.
J Cardiovasc Comput Tomogr (2009) 3. Supplement 1, S13-S22"This practice equates with ineffective resource utilization, increased health care costs, and unnecessary radiation and contrast exposure."
CT Angiography in the Evaluation of Acute Pulmonary Embolus
Costantino MM et al.
AJR 2008; 191;471-474"Our data showed suboptimal use of the Wells criteria and subjective overestimation of the probability of PE before ordering of CTA. Although a definitive acceptable PE positivity rate for CTA has not been established, the 10% yield represents overuse of CTA as a screening rather than diagnostic examination."
CT Angiography in the Evaluation of Acute Pulmonary Embolus
Costantino MM et al.
AJR 2008; 191;471-474- Current Standard of Care for Low Risk Chest Pain Patients
- Serial cardiac enzymes
- Serial ECGs
- Cardiac stress test
- This may take up to 30 hours to complete and charges are high in the 8,000 dollar range "In low risk patients with chest pain, discharge from the emergency department based on negative cardiac CT, enzyme tests, and ECG may signifiicantly decrease both length of stay and hospital charges compared with the standard of care."
Low-Risk Patients With Chest Pain in the Emergency Deprtment: Negative 64-MDCT Coronary Angiography May Reduce Length of Stay and Hospital Charges
May JH et al
AJR 2009; 193:150-154- Triple Rule Out Protocol
- Scan is from above arch (1-2 cm) thru the base of the heart
- CT angiography begins 5 seconds after contrast reaches the left atrium (64 MDCT)
- Injection is biphasic with 70 ml of iodine 350 followed by 50 ml of diluted contrast (25 ml of iodine 350 and 25 ml saline)
- Beta blockers critical
Triple-Rule-Out CT Angiography for Evaluation of Acute Chest Pain and Possible Acute Coronary Syndrome
Halpern EJ
Radiology 2009; 252:332-345
"The primary goal of triple-rule-out CT in the emergency department is to facilitate the safe rapid discharge of patients judged to be at low to intermediate risk of acute coronary syndrome."
Triple-Rule-Out CT Angiography for Evaluation of Acute Chest Pain and Possible Acute Coronary Syndrome
Halpern EJ
Radiology 2009; 252:332-345"Triple-rule-out (TRO) computed tomographic angiography can provide cost effective evaluation of the coronary arteries, aorta, pulmonary arteries, an adjacent intrathoracic structures for the patient with acute chest pain. TRO CT is most appropriate for the patient who is judged to be at low to intermediate risk for acute coronary syndrome and whose symptoms may also be attributable to acute pathologic conditions of the aorta or pulmonary arteries."
Triple-Rule-Out CT Angiography for Evaluation of Acute Chest Pain and Possible Acute Coronary Syndrome
Halpern EJ
Radiology 2009; 252:332-345- Why do adult patients visit the ER?
- Chest pain
- Abdominal pain
- Back pain
- Headache
- Shortness of breath
- This list if for patients over 15 years of age - Triple Rule-Out CT Protocol
- 64 MDCT Scanner
- Cephalic to caudal direction scanning
- 130 cc of contrast injected over 66 seconds (80 cc at 5 cc/sec, 50 cc at 2 cc/sec, then 50 cc saline at 2 cc/sec)
- Triple Rule-out and Dedicated Coronary Artery CTA: Comparison of Coronary Image Quality Rahmani N, Jeudy J, White CS Acad Radiol 2009; 16:604-609 "The image quality of triple rule out CTA is comparable to that of dedicated coronary CTA, showing no statistically significant difference in motion artifacts or opacification, and therefore may be alternative and useful diagnostic study in a select group of emergency patients."
Triple Rule-out and Dedicated Coronary Artery CTA: Comparison of Coronary Image Quality
Rahmani N, Jeudy J, White CS
Acad Radiol 2009; 16:604-609- Triple Rule-Out CT Protocol
- Dual Source CT Scanner
- 110 ml of contrast injected at 4 cc/sec followed by 30 ml of saline
- Trigger set in ascending aorta
- Scanning was done in a cranial caudal direction
- Triple Rule-Out CT in Patients with Suspicion of Acute Pulmonary Embolism: Findings and Accuracy Schertler T et al. Acad Radiol 2009; 16:708-717 "Triple rule-out CT is feasible in patients with suspicion of PE, reveals a wide range of vascular and non-vascular chest disease, and offers an excellent overall diagnostic performance."
Triple Rule-Out CT in Patients with Suspicion of Acute Pulmonary Embolism: Findings and Accuracy
Schertler T et al.
Acad Radiol 2009; 16:708-717- Chronic Pulmonary Thromboembolism: Collateral Systemic Supply
- Dilated bronchial arteries
- Bronchial artery blood flow is usually 1-2% of cardiac output, in chronic thromboembolic pulmonary hypertension it is up to 30% of systemic blood flow - Chronic Pulmonary Thromboembolism: Pulmonary Hypertension
- Main pulmonary artery diameter of greater than 29 mm
- When the ratio of main pulmonary artery to the aorta is greater than 1:1 there is a strong correlation with elevated pulmonary artery pressure in patients younger than 50 years of age - Chronic Pulmonary Thromboembolism: Direct Pulmonary Arterial Signs
- Complete obstruction
- Partial filling defects
- Bands and webs
- Calcified thrombus - Chronic Pulmonary Thromboembolism: Vascular Signs
- Direct Pulmonary Arterial Signs
- Signs due to pulmonary hypertension
- Signs due to systemic collateral supply "In summary, initial investigations suggest that CT angiography has considerable potential to streamline chest pain evaluation in the ED, but further investigation is imperative to establish its precise role."
Chest Pain in the Emergency Department: Role of Multidetector CT
White CS, Kuo D
Radiology 2007; 245:672-681- Coronary Artery Aneurysms: Etiology
- Congenital
- Acquired
–Atherosclerosis
–Trauma
–Post angioplasty (procedure related)
–Arteritis
–Kawasaki’s disease
–Connective tissue disease (Marfan’s, Lupus, etc.)
- Coronary Artery Aneurysms: Management
- Conservative management (watchful waiting)
- Bypass grafts
- Covered stent placement
- Coronary Artery Fistulae: Facts
- 0.1-0.2% of patients undergoing cardiac cath
- Right coronary artery most commonly involved
- Drainage much more common to right side of the heart
- Can result in myocardial ischemia
- Coronary Artery Aneurysms: Facts
- Most common causes are atherosclerotic,congenital and mycotic-embolic disease
- Kawasaki’s disease has giant aneurysms and up to 25% of patient with acute Kawasaki’s disease will develop aneurysms
- Triple Chest Pain Protocol
- Acute coronary ischemia and myocardial infarction
- Aortic dissection
- Pulmonary embolism
- MDCT of Myocardial Infarction
- Repeat study 5 minutes after contrast injection (delayed phase imaging)
- Hypoenhancement zone (ischemic zone) may only be seen at this point
- Myocardial Infarction:CT Findings
- Early hypodensity in the myocardium
- Persistent hypodensity in the myocardium
- Delayed enhancement of area of hypodensity seen on early phase imaging (first pass).
- This may be in the periphery
- " CT coronary angiography using a 16-MDCT scanner enables accurate noninvasive detection of significant coronary artery disease in patients hospitalized for acute chest pain syndrome."
16-MDCT Coronary Angiography versus Invasive Coronary Angiography in Acute Chest Pain Syndrome: A Blinded Prospective Study
Ghersin E et al.
AJR 2006; 186:177-184
- Acute Chest Pain: Possibilities
- Pulmonary Embolism
- Aortic dissection
- Coronary artery disease
- Pneumonia
- Pleural effusions
- "ECG-gated MDCT appears to be logistically feasible and shows promise as a comprehensive method for evaluating cardiac and noncardiac chest pain in stable emergency department patients."
Chest Pain Evaluation in the Emergency Department: Can MDCT Provide a Comprehensive Evaluation? White CS et al. AJR 2005; 185:533-540
- "Sensitivity and specificity for the establishment of a cardiac cause of chest pain were 83% and 96% respectively. Overall sensitivity and specificity for all other cardiac and noncardiac causes were 87% and 96% respectively."
Chest Pain Evaluation in the Emergency Department: Can MDCT Provide a Comprehensive Evaluation? White CS et al. AJR 2005; 185:533-540
- "The chest pain protocol can be used to assess both the pulmonary arteries and the thoracic aorta, whereas the ECG-gating protocol appears to be a promising adjunct for a comprehensive single chest pain protocol."
MDCT Angiography of Acute Chest Pain: Evaluation of ECG-Gated and Nongated Techniques
Raptopoulos VD et al.
AJR 2006; 186:S346-S356k. - "The daily use of MDCT studies for the evaluation of pulmonary embolic disease or aortic abnormalities can reveal incidental PDAs. Small incidental PDAs can be identified on chest MDCT angiography timed for either the pulmonary arteries or the aorta."
Incidental Finding on MDCT of Patent Ductus Arteriosus: Use of CT and MRI to Assess Clinical Importance
Goitein O et al.
AJR 2005;184:1924-1931