Imaging Pearls ❯ April 2024
|
-- OR -- |
|
3D and Workflow
- Cinematic rendering (CR) is a novel CT post-processing technique that utilizes advanced light modeling to generate highly photorealistic anatomic visualization. This generates unique prospects in the evaluation of adrenal masses. As one of the first large tertiary care centers to incorporate CR into routine diagnostic workup, our preliminary experience with using CR has been positive, and we have found CR to be a valuable adjunct during surgical planning. Herein, we highlight the unique utility of CR techniques in the workup of adrenal lesions and provide commentary on the opportunities and obstacles associated with the application of this novel display method in this setting.
Three-dimensional CT cinematic rendering of adrenal masses: Role in tumor analysis and management.
Ahmed TM, Rowe SP, Fishman EK, Soyer P, Chu LC.
Diagn Interv Imaging. 2024 Jan;105(1):5-14. - “Recently, a novel method of 3D visualization, known as cinematic rendering (CR) has been introduced. While CR shares many similarities with VR, it utilizes a more complex global lighting model that incorporates elements of ray tracing and scatter to generate images that are photorealistic. Through more realistically modeling the complex interactions of photons passing through the imaged volume, CR images attain improved levels of surface detail and shadow realism. CR also allows for highly adjustable real-time post processing and windowing, enabling tailored visualization of any given region of interest, its vascular supply, and its adjacent structures. n region of interest, its vascular supply, and its adjacent structures. ”
Three-dimensional CT cinematic rendering of adrenal masses: Role in tumor analysis and management.
Ahmed TM, Rowe SP, Fishman EK, Soyer P, Chu LC.
Diagn Interv Imaging. 2024 Jan;105(1):5-14. - “Pheochromocytomas are neuroendocrine tumors that arise from the chromaffin cells of the adrenal medulla and are present in 0.1% to 0.2% of adults with hypertension. Although typically associated with the triad of new-onset, refractory or paroxysmal hypertension, palpitations, and headache, up to 10% of patients may remain asymptomatic. Pheochromocytomas have a number of syndromic associations, most notably multiple endocrine neoplasia 2, von Hippel-Lindau syndrome, neurofibromatosis, Sturge-Weber syndrome, and tuberous sclerosis. While the up to 95% of pheochromocytomas are typically benign, 10%–15% may be malignant. Diagnosis is established on the basis of elevated urinary and plasma fractioned metanephrines and catecholamines alongside characteristic imaging features. ”
Three-dimensional CT cinematic rendering of adrenal masses: Role in tumor analysis and management.
Ahmed TM, Rowe SP, Fishman EK, Soyer P, Chu LC.
Diagn Interv Imaging. 2024 Jan;105(1):5-14. - “CR visualizations in the workup of pheochromocytomas can accentuate the dynamic enhancement pattern through more distinctly highlighting the anatomy of the enhanced components within the mass .Additionally, CR confers the added benefit of dynamic window width and level adjustment, which can aid in delineating cystic regions and septations within the tumor. Beyond tissue characterization, CR vascular mapping can also potentially improve visualization of the vascular supply, which is especially important in laparoscopic resection of vascular tumors such as pheochromocytomas. It can also be useful for surgical planning of adrenal sparing procedures.”
Three-dimensional CT cinematic rendering of adrenal masses: Role in tumor analysis and management.
Ahmed TM, Rowe SP, Fishman EK, Soyer P, Chu LC.
Diagn Interv Imaging. 2024 Jan;105(1):5-14. - “ACC is a highly malignant neoplasm arising from the adrenal cortex ACC is a rare tumor with an annual incidence of 0.5–2 per million per year that peaks in the fourth and fifth decades of life, with a slight female preponderance. ACC can present as either a functional or nonfunctional tumor. Sixty p. cent of ACCs are functional and present with characteristic clinical manifestations, with Cushing syndrome being the most common manifestation . Alternatively, patients with nonfunctional tumors most commonly present with pain, a palpable mass or gastrointestinal complaints . Thirty p. cent of (nonfunctional ACCs present with metastatic disease at detection, due to their late presentation .”
Three-dimensional CT cinematic rendering of adrenal masses: Role in tumor analysis and management.
Ahmed TM, Rowe SP, Fishman EK, Soyer P, Chu LC.
Diagn Interv Imaging. 2024 Jan;105(1):5-14. - “Soft tissue sarcomas (STS) are a heterogenous group of mesenchymal tumors [28]. While STS can arise virtually anywhere within the body, involvement of the adrenals is exceedingly rare, and ascertaining definitive epidemiological data on adrenal involvement is difficult. Prior retrospective reviews have reported STSs to account for only 1.3% of all adrenal tumors . Among adult STSs, undifferentiated pleomorphic sarcoma, liposarcoma and leiomyosarcoma are the most common histological subtypes and typically present in the elderly. Typically, undifferentiated pleomorphic sarcoma appears as heterogenous soft tissue masse with irregular margins and attenuate similarly to muscle. Soft tissue areas within the mass enhance following intravenous administration of contrast material. Areas of decreased attenuation, representing hemorrhage and necrosis, are often centrally present, which can complicate radiological differentiation from ACC .”
Three-dimensional CT cinematic rendering of adrenal masses: Role in tumor analysis and management.
Ahmed TM, Rowe SP, Fishman EK, Soyer P, Chu LC.
Diagn Interv Imaging. 2024 Jan;105(1):5-14. - “Pancreatic neuroendocrine tumours (PNETs) are a rare subset of pancreatic tumours that have historically comprised up to 3% of all clinically detected pancreatic tumours. In recent decades, however, advancements in imaging have led to an increased incidental detection rate of PNETs and imaging has played an increasingly central role in the initial diagnostics and surgical planning of these tumours. Cinematic rendering (CR) is a 3D post-processing technique that generates highly photorealistic images through more realistically modelling the path of photons through the imaged volume. This allows for more comprehensive visualization, description, and interpretation of anatomical structures. In this 2-part review article, we present the first description of the various CR appearances of PNETs in the reported literature while providing commentary on the unique clinical opportunities afforded by the adjunctive utilization of CR in the workup of these rare tumours.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 1: Tumour Detection and Characterization
Ahmed TM, Fishman EK, Chu LC.
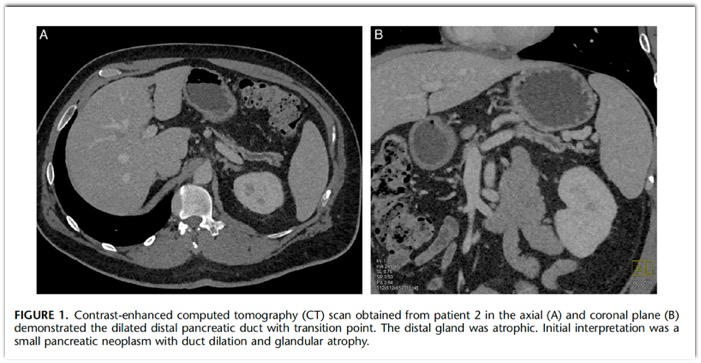
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - At CT, PNETs typically appear as well circumscribed avidly enhancing masses that may arise from any portion of the pancreas. Enhancement patterns for small PNETs are usually uniform, and some may present with a characteristic rim enhancement that can help clue in the diagnosis. The degree and homogeneity of lesion enhancement is correlated with tumour grade, and among larger PNETs, which predominantly consist of non-hyperfunctioning variants, the presence of cystic degeneration, intralesional necrosis and calcification can result in an inhomogeneous pattern of enhancement. PNETs are classically best visualized in the arterial phase. While smaller PNETs can be particularly difficult to see on venous or delayed images, a small proportion of PNETs may atypically be better visualized on portal venous phase imaging.
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 1: Tumour Detection and Characterization
Ahmed TM, Fishman EK, Chu LC.
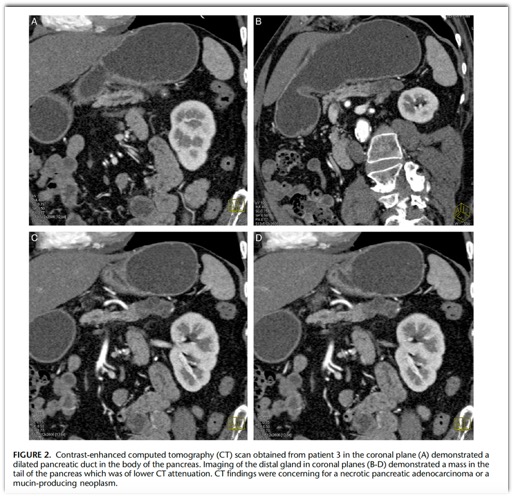
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - Differential diagnoses of PNETs consist of pancreatic metastases, most often from renal cell carcinoma, solid variant serous cystadenoma, peripancreatic gastrointestinal stromal tumour, and intrapancreatic accessory spleen.5 In rarer cases of hypovascular PNETs, differentiation from adenocarcinoma is essential and carries significant implications for management.
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 1: Tumour Detection and Characterization
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - “Cinematic rendering may allow for the detection of the presence of tumour in cases where subtle textural changes due to inherent differences between normal and abnormal tissue are present, but a defined mass is not yet visible. Through this, CR can potentially facilitate early disease detection and help differentiate PNETs from normal pancreatic parenchyma. CR can similarly assist in differentiating PNETs from intrapancreatic accessory spleens through accentuating textural differences that may not be appreciable at non-cinematic imaging . Display configurations of CR may also be manipulated to conceal uninvolved pancreatic parenchyma, allowing for isolated visualization of PNETs. This can make tumours remarkably conspicuous as well as highlight the spatial relationship of the tumour with extra-pancreatic anatomy.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 1: Tumour Detection and Characterization
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - “While PNETs are typically solid tumours, the presence of cystic internal components is not uncommon, with up to 10% of PNETs being purely cystic. Cystic components in PNETs are most often encountered among larger PNETs that undergo cystic degeneration or necrosis. Rarely, small PNETs with cystic change are also encountered and can pose diagnostic challenges. Purely cystic PNETs generally exhibit more indolent behaviour and carry more favourable prognoses, which has also led to the rise of conflicting opinions regarding the value of resection in these cases.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 1: Tumour Detection and Characterization
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - “Purely cystic PNETs generally exhibit more indolent behaviour and carry more favourable prognoses, which has also led to the rise of conflicting opinions regarding the value of resection in these cases.19 Simultaneously however, cystic PNET can be misdiagnosed as a potentially malignant cystic lesion (ie, mucinous cystic neoplasm, intraductal papillary neoplasm) that ought to be resected, or a benign cystic lesion (ie, serous cystadenoma) for which surgery is not indicated, which can lead to suboptimal patient outcomes. Radiological characterization of the internal architecture of these tumours is therefore particularly important due to the wide range of potential implications upon management.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 1: Tumour Detection and Characterization
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - “Purely cystic PNETs generally exhibit more indolent behaviour and carry more favourable prognoses, which has also led to the rise of conflicting opinions regarding the value of resection in these cases.19 Simultaneously however, cystic PNET can be misdiagnosed as a potentially malignant cystic lesion (ie, mucinous cystic neoplasm, intraductal papillary neoplasm) that ought to be resected, or a benign cystic lesion (ie, serous cystadenoma) for which surgery is not indicated, which can lead to suboptimal patient outcomes. Radiological characterization of the internal architecture of these tumours is therefore particularly important due to the wide range of potential implications upon management.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 1: Tumour Detection and Characterization
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - “Cinematic rendering is uniquely suited to visualization of these cases through its ability to greatly improve depth perception. Improved depth perception, in conjunction with dynamic textural visualization of CR may allow for optimal characterization of the internal architecture of cystic components. This can result in superior visualization of fine internal septations and mural nodularity within these lesions that may help in differentiating them from other cystic pancreatic lesions. In particular, the presence of an avidly enhancing hypervascular rim, owing to the rich blood supply of PNETs, is known to be a highly suggestive radiologic feature of cystic PNETs. Improved characterization of the cystic mural interface using CR may be especially advantageous in appreciating this key finding.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 1: Tumour Detection and Characterization
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. 
- “Precise evaluation of the presence and extent of vascular invasion is essential in determining the resectability of PNETs and to plan for possible vascular reconstruction. Though CT is considered to have excellent sensitivity in identifying major vessel involvement, prior studies have found that 25% to 50% of patients with PNETs who are radiologically determined to have vascular invasion, are confirmed to have true vascular invasion at the time of surgery. On the more concerning flipside of this, it is similarly possible that patients with softer radiological signs of vascular invasion may be denied surgery due to perceived vascular involvement in the absence of true involvement. In these equivocal cases, vascular abutment may be misinterpreted as vascular encasement and vice versa. CR may alleviate the diagnostic burden in these cases by generating exquisitely detailed vascular maps that allow radiologists to visualize the tumour-vessel interface with increased confidence. Through this, it may be possible to differentiate vascular stretching, abutment, and compression from true vessel invasion. Radiological assessment of vascular involvement in PNETs is also uniquely nuanced as PNETs may not traditionally encase vessels but instead tend to invade and expand venous vasculature.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 2: Preoperative Planning and Evaluation of Metastatic Disease.
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - “Unlike PDAC, the presence of hepatic metastases in PNETs does not preclude surgical resection, and potentially curative resection of the primary tumour and metastatic hepatic implants is still possible in up to 25% of patients.14 Timely radiological identification of hepatic metastases and subsequent deliberation of their resectability is therefore critical to the management of metastatic PNETs. Using CR, rendering parameters can be modified to either highlight the characteristically hypervascular metastases but may also be adjusted to optimize visualization in cases of atypical hypovascular-appearing metastases. Display settings can also be further modified to render the background hepatic parenchyma translucent to further accentuate any hepatic metastases. Once lesions are identified, the enhanced depth perception of CR can also help differentiate them from benign liver lesions through improving visualization of their internal architecture. “
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 2: Preoperative Planning and Evaluation of Metastatic Disease.
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - “CR augmentation also has the potential to go beyond optimizing disease detection and classification and may also impact surgical planning. This is achieved through the generation of photorealistic images that essentially serve as personalized anatomic models for the operating team. Anecdotally, pancreatic surgeons at our institution have found these reconstructions helpful for preoperative planning and in improving intraoperative situational awareness. This is particularly relevant in cases of laparoscopic surgery, where real-time intraoperative visualization is restricted.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 2: Preoperative Planning and Evaluation of Metastatic Disease.
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - “While CR has shown promise in enhancing the diagnostics and surgical planning of PNETs in our institution, there remain certain limitations that hinder broader adoption. One significant constraint revolves around the specialized expertise required to generate CR images. Optimization of CR images is crucial to accurately represent the anatomy and pathology of interest. This task demands the dedicated training of radiologists who need to customize the display settings for each specific pathology. Using incorrect parameters can impede visualization and may result in incorrect diagnoses. This is compounded by the shadowing effects generated by the CR global lighting model which if not duly accounted for may potentially obscure visualization of significant pathology. As CR becomes more widely adopted, this aspect of CR is anticipated to become more standardized and perhaps even automated.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 2: Preoperative Planning and Evaluation of Metastatic Disease.
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - “CR holds promising potential for enhancing the diagnostics and surgical planning of PNETs. Part 2 of this pictorial review highlights the utility of CR in vascular mapping, preoperative planning, and evaluation of metastatic disease of PNETs. In the words of Dr. O’Brien, cinematic rendering, though still in its infancy, is an exciting technique; future studies investigating implementation of CR into clinical practice have potential to add great value to our practice.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 2: Preoperative Planning and Evaluation of Metastatic Disease.
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705.


Adrenal
- “Prompt diagnosis may matter clinically because 16– 50% of patients with bilateral adrenal hemorrhage eventually have life-threatening adrenal insufficiency. Recognition of adrenal hemorrhage secondary to underlying tumor is also important so that potentially dangerous masses such as pheochromocytoma do not go untreated. Despite the importance of adrenal hemorrhage and the critical role of imaging, relatively little has been published on this topic in the radiologic literature.”
Imaging of Nontraumatic Adrenal Hemorrhage
Eric Jordan et al.
AJR 2012; 199:W91–W98 - “The causes of nontraumatic adrenal hemorrhage include stress; bleeding diatheses, including anticoagulant use; procedures; and intratumoral bleeding. Stress includes recent surgery, organ failure, sepsis, and pregnancy. These causes are not mutually exclusive and can coexist. Recognition of adrenal hemorrhage is particularly important because of the common use of anticoagulation and the introduction of agents such as dabigatran. Noniatrogenic bleeding diathesis such as disseminated intravascular coagulopathy and antiphospholipid syndrome can also lead to adrenal hemorrhage.”
Imaging of Nontraumatic Adrenal Hemorrhage
Eric Jordan et al.
AJR 2012; 199:W91–W98 - “Acute intratumoral adrenal hemorrhage is most commonly seen in pheochromocytoma, but hemorrhage has also been described in myelolipomas, metastatic lesions, adrenocortical carcinomas, adenomas, and hemangiomas. Interestingly, calcification suggestive of previous hemorrhage was seen in 26% of myelolipomas (22 of 86) in one study, but these tumors seem to rarely present with clinically overt hemorrhage.”
Imaging of Nontraumatic Adrenal Hemorrhage
Eric Jordan et al.
AJR 2012; 199:W91–W98 - “Other features that may be seen in acute adrenal hemorrhage include periadrenal infiltration, active extravasation with retroperitoneal bleeding, and maintenance of an adreniform shape. Unenhanced CT in isolation, performed either because adrenal hemorrhage is suspected clinically or because of a contraindication to IV contrast administration, may show adrenal enlargement of greater than simple fluid attenuation and periadrenal infiltration.”
Imaging of Nontraumatic Adrenal Hemorrhage
Eric Jordan et al.
AJR 2012; 199:W91–W98 - “Bleeding often continues until the adrenal gland expands beyond the adreniform shape and forms a round or oval hematoma in the gland. The size of hematomas varies, ranging from a few centimeters to well over 10 cm. A hematoma appears on CT images as a circular nonenhancing mass of greater than simple fluid attenuation (e.g., 50–90 HU). Occasionally, extravasation of contrast material during catheter angiography or venous sampling or prior injection of contrast material for cystography results in an appearance resembling acute adrenal hemorrhage, but correlation with the history should help with the distinction.”
Imaging of Nontraumatic Adrenal Hemorrhage
Eric Jordan et al.
AJR 2012; 199:W91–W98 - “Over time, the size and CT attenuation of adrenal hemorrhage decrease, eventually reaching simple fluid attenuation or even complete resolution. The time course of these changes in nontraumatic adrenal hemorrhage has not been well described, but shrinkage and decreased attenuation were seen in most of 35 traumatic adrenal hemorrhages evaluated with repeat CT after a mean interval of 19 days.”
Imaging of Nontraumatic Adrenal Hemorrhage
Eric Jordan et al.
AJR 2012; 199:W91–W98 - “Later, chronic hemorrhage may appear as adrenal atrophy or a hemorrhagic adrenal pseudocyst. Atrophy appears on CT images as a shriveled, isoattenuating adreniform structure. A hemorrhagic adrenal pseudocyst is a chronic organized collection of hemorrhage that presents as nonenhancing, thin-rimmed cystic structures. At CT, pseudocysts are nonenhancing and have central hypoattenuation close to that of simple fluid”
Imaging of Nontraumatic Adrenal Hemorrhage
Eric Jordan et al.
AJR 2012; 199:W91–W98 - “The frequency with which adrenal hemorrhage is associated with an underlying adrenal tumor has not been well described, although our experience suggests this type of hemorrhage is a relatively rare occurrence. The distinction of tumoral from nontumoral hemorrhage is straightforward when a neoplastic mass can be appreciated within or adjacent to a hematoma, but finding the mass can be difficult or impossible, particularly in the acute phase.”
Imaging of Nontraumatic Adrenal Hemorrhage
Eric Jordan et al.
AJR 2012; 199:W91–W98 - “The rapid development or evolution of a nonenhancing adrenal mass or masses that retain an adreniform shape or have high T1 signal intensity at MRI of a patient under stress or with a bleeding diathesis should suggest acute adrenal hemorrhage. Bilateral hemorrhage can cause life-threatening adrenal insufficiency. Chronic hemorrhage may appear at imaging as a thin-walled adrenal pseudocyst or adrenal atrophy. Imaging findings that suggest underlying tumor as a cause of adrenal hemorrhage are intralesional calcification, enhancement, and hypermetabolic activity on PET images.”
Imaging of Nontraumatic Adrenal Hemorrhage
Eric Jordan et al.
AJR 2012; 199:W91–W98 - The majority of cases of adrenal trauma do not display specific signs and symptoms; however, the presence of adrenal trauma may indicate the presence of severe trauma and should prompt an evaluation for associated injuries. Due to the possible life-threatening events associated with adrenal injuries, several authors have advised aggressive management and early intervention to avoid complications such as delayed adrenal insufficiency. In contrast, an increasing number of studies have reported that conservative management can be used for patients with adrenal trauma.
Adrenal Gland Trauma: An Observational Descriptive Analysis from a Level 1-Trauma Center.
Al-Thani H, et al.
J Emerg Trauma Shock. 2021 Apr-Jun;14(2):92-97. - “Adrenal hematomas with a mass-like configuration offer a potential diagnostic dilemma for radiologists and surgeons. Although it is rare that an adrenal hemorrhage is surgically resected, awareness of the potential appearances of these lesions is important to spare patients from unnecessarily aggressive surgery.”
Computed Tomography Appearance of Surgically Resected Adrenal Hematomas.
Rowe SP, Mathur A, Bishop JA, Epstein JI, Prescott JD, Salvatori R, Siegelman SS, Fishman EK.
J Comput Assist Tomogr. 2016 Nov/Dec;40(6):892-895. - “Incidental adrenal lesions are found in 2% to 10% of the population. The presence and pattern of calcifications, in conjunction with other clinical and imaging features, such as soft tissue attenuation, enhancement, and laterality, can aid in narrowing a differential diagnosis, thereby preventing unnecessary biopsies and avoiding delays in management. Calcified adrenal lesions can be categorized under the clinical and laboratory headings of normal adrenal function, hyperfunctioning adrenal tissue, and adrenal insufficiency.”
Calcified Adrenal Lesions: Pattern Recognition Approach on Computed Tomography With Pathologic Correlation.
Consul, Nikita MD et al.
Journal of Computer Assisted Tomography 44(2):p 178-187, 3/4 2020
- Cinematic rendering (CR) is a novel CT post-processing technique that utilizes advanced light modeling to generate highly photorealistic anatomic visualization. This generates unique prospects in the evaluation of adrenal masses. As one of the first large tertiary care centers to incorporate CR into routine diagnostic workup, our preliminary experience with using CR has been positive, and we have found CR to be a valuable adjunct during surgical planning. Herein, we highlight the unique utility of CR techniques in the workup of adrenal lesions and provide commentary on the opportunities and obstacles associated with the application of this novel display method in this setting.
Three-dimensional CT cinematic rendering of adrenal masses: Role in tumor analysis and management.
Ahmed TM, Rowe SP, Fishman EK, Soyer P, Chu LC.
Diagn Interv Imaging. 2024 Jan;105(1):5-14. - “Recently, a novel method of 3D visualization, known as cinematic rendering (CR) has been introduced. While CR shares many similarities with VR, it utilizes a more complex global lighting model that incorporates elements of ray tracing and scatter to generate images that are photorealistic. Through more realistically modeling the complex interactions of photons passing through the imaged volume, CR images attain improved levels of surface detail and shadow realism. CR also allows for highly adjustable real-time post processing and windowing, enabling tailored visualization of any given region of interest, its vascular supply, and its adjacent structures. n region of interest, its vascular supply, and its adjacent structures. ”
Three-dimensional CT cinematic rendering of adrenal masses: Role in tumor analysis and management.
Ahmed TM, Rowe SP, Fishman EK, Soyer P, Chu LC.
Diagn Interv Imaging. 2024 Jan;105(1):5-14. - “Pheochromocytomas are neuroendocrine tumors that arise from the chromaffin cells of the adrenal medulla and are present in 0.1% to 0.2% of adults with hypertension. Although typically associated with the triad of new-onset, refractory or paroxysmal hypertension, palpitations, and headache, up to 10% of patients may remain asymptomatic. Pheochromocytomas have a number of syndromic associations, most notably multiple endocrine neoplasia 2, von Hippel-Lindau syndrome, neurofibromatosis, Sturge-Weber syndrome, and tuberous sclerosis. While the up to 95% of pheochromocytomas are typically benign, 10%–15% may be malignant. Diagnosis is established on the basis of elevated urinary and plasma fractioned metanephrines and catecholamines alongside characteristic imaging features. ”
Three-dimensional CT cinematic rendering of adrenal masses: Role in tumor analysis and management.
Ahmed TM, Rowe SP, Fishman EK, Soyer P, Chu LC.
Diagn Interv Imaging. 2024 Jan;105(1):5-14. - “CR visualizations in the workup of pheochromocytomas can accentuate the dynamic enhancement pattern through more distinctly highlighting the anatomy of the enhanced components within the mass .Additionally, CR confers the added benefit of dynamic window width and level adjustment, which can aid in delineating cystic regions and septations within the tumor. Beyond tissue characterization, CR vascular mapping can also potentially improve visualization of the vascular supply, which is especially important in laparoscopic resection of vascular tumors such as pheochromocytomas. It can also be useful for surgical planning of adrenal sparing procedures.”
Three-dimensional CT cinematic rendering of adrenal masses: Role in tumor analysis and management.
Ahmed TM, Rowe SP, Fishman EK, Soyer P, Chu LC.
Diagn Interv Imaging. 2024 Jan;105(1):5-14. - “ACC is a highly malignant neoplasm arising from the adrenal cortex ACC is a rare tumor with an annual incidence of 0.5–2 per million per year that peaks in the fourth and fifth decades of life, with a slight female preponderance. ACC can present as either a functional or nonfunctional tumor. Sixty p. cent of ACCs are functional and present with characteristic clinical manifestations, with Cushing syndrome being the most common manifestation . Alternatively, patients with nonfunctional tumors most commonly present with pain, a palpable mass or gastrointestinal complaints . Thirty p. cent of (nonfunctional ACCs present with metastatic disease at detection, due to their late presentation .”
Three-dimensional CT cinematic rendering of adrenal masses: Role in tumor analysis and management.
Ahmed TM, Rowe SP, Fishman EK, Soyer P, Chu LC.
Diagn Interv Imaging. 2024 Jan;105(1):5-14. - Soft tissue sarcomas (STS) are a heterogenous group of mesenchymal tumors [28]. While STS can arise virtually anywhere within the body, involvement of the adrenals is exceedingly rare, and ascertaining definitive epidemiological data on adrenal involvement is difficult. Prior retrospective reviews have reported STSs to account for only 1.3% of all adrenal tumors . Among adult STSs, undifferentiated pleomorphic sarcoma, liposarcoma and leiomyosarcoma are the most common histological subtypes and typically present in the elderly [41]. Typically, undifferentiated pleomorphic sarcoma appears as heterogenous soft tissue masse with irregular margins and attenuate similarly to muscle. Soft tissue areas within the mass enhance following intravenous administration of contrast material. Areas of decreased attenuation, representing hemorrhage and necrosis, are often centrally present, which can complicate radiological differentiation from ACC .”
Three-dimensional CT cinematic rendering of adrenal masses: Role in tumor analysis and management.
Ahmed TM, Rowe SP, Fishman EK, Soyer P, Chu LC.
Diagn Interv Imaging. 2024 Jan;105(1):5-14. - “CR has promising potential in the characterization of adrenal masses and can influence surgical planning. CR can potentially improve the appreciation of the spatial relationship between the adrenal mass and adjacent structures and delineation of the major vascular supply. Enhanced surgical planning is particularly important with laparoscopic surgeries, in which the surgeons’ real-time intraoperative visualization may be limited. Results from preliminary studies applying cinematic rendering to imaging of non-adrenal pathology to assess clinical benefit have been promising .In one study, orthopedic surgeons and radiologists performed significantly better in the assessment of pelvic instability when using combined dual-energy CT with cinematic rendering (AUC = 0.82) over single-energy CT alone (AUC = 0.67). While this generates optimism, and is in agreement with our initial institutional observations of using CR, a prior study reported that radiologists, in fact, had lower accuracy in diagnosing vascular invasion in deep soft tissue sarcomas with CR imaging compared to standard contrast-enhanced axial imaging and VR imaging.”
Three-dimensional CT cinematic rendering of adrenal masses: Role in tumor analysis and management.
Ahmed TM, Rowe SP, Fishman EK, Soyer P, Chu LC.
Diagn Interv Imaging. 2024 Jan;105(1):5-14.
Cardiac
- “Additionally, nearly all young persons (men age <50 years and women age <60 years) who do not smoke or have diabetes have a low 10-year risk for ASCVD based on traditional risk factors. However, there is increasing awareness of the utility for CAC scoring in this age group and of the importance of reporting the presence of any CAC given the high lifetime risk for ASCVD.”
Incidental Coronary Artery Calcium: Nothing Is More Expensive Than a Missed Opportunity.
Blumenthal RS, Grant J, Whelton SP.
J Am Coll Cardiol. 2023 Sep 19;82(12):1203-1205. - However, this study demonstrates that by using artificial intelligence deep learning algorithms, we can easily quantify and measure CAC from noncardiac CT chest scans without any additional monetary or radiation-related cost to the patient. These results highlight the underutilization of this “free” information and demonstrate a real-world, high-impact use for AI algorithms that is ready right now to directly improve patient care. The pragmatic use of this AI algorithm and increased uptake for reporting of incidental CAC has the potential to transform the appropriate allocation of primary prevention medications, motivate asymptomatic adults to make sustained lifestyle improvements, reduce the burden of ASCVD, and potentially reverse the recent trend of increased ASCVD in the United States.
Incidental Coronary Artery Calcium: Nothing Is More Expensive Than a Missed Opportunity.
Blumenthal RS, Grant J, Whelton SP.
J Am Coll Cardiol. 2023 Sep 19;82(12):1203-1205. - Background: Coronary artery calcium (CAC) has prognostic value for major adverse cardiovascular events (MACE) in asymptomatic individuals, whereas its role in symptomatic patients is less clear.
Purpose: To assess the prognostic value of CAC scoring for MACE in participants with stable chest pain initially referred for invasive coronary angiography (ICA).
Conclusion: In participants with stable chest pain initially referred for ICA, a CAC score of 0 showed very low risk of MACE, and higher CAC scores showed increasing risk of obstructive CAD, revascularization, and MACE at follow-up.
Coronary Artery Calcium Score Predicts Major Adverse Cardiovascular Events in Stable Chest Pain
The DISCHARGE Trial Group
Radiology 2024; 310(3):e231557 - Purpose: To assess the prognostic value of CAC scoring for MACE in participants with stable chest pain initially referred for invasive coronary angiography (ICA).
Materials and Methods: This prespecified subgroup analysis from the Diagnostic Imaging Strategies for Patients With Stable Chest Pain and Intermediate Risk of Coronary Artery Disease (DISCHARGE) trial, conducted between October 2015 and April 2019 across 26 centers in 16 countries, focused on adult patients with stable chest pain referred for ICA. Participants were randomly assigned to undergo either ICA or coronary CT. CAC scores from noncontrast CT scans were categorized into low, intermediate, and high groups based on scores of 0, 1–399, and 400 or higher, respectively. The end point of the study was the occurrence of MACE (myocardial infarction, stroke, and cardiovascular death) over a median 3.5-year follow-up, analyzed using Cox proportional hazard regression tests
Coronary Artery Calcium Score Predicts Major Adverse Cardiovascular Events in Stable Chest Pain
The DISCHARGE Trial Group
Radiology 2024; 310(3):e231557 - Key Results
■ In a prospective study of 1749 participants with stable chest pain followed up for 3.5 years, those with a coronary artery calcium (CAC) score of 0 at CT had a lower prevalence of obstructive coronary artery disease (4.1%) than participants with a CAC score of 400 or higher (76.1%; P < .001).
■ The major adverse cardiovascular events rate was lower in participants with a CAC score of 0 (0.5%; hazard ratio [HR], 0.08) than a CAC score of 400 or higher (6.8%; HR, 1 [reference]; P < .001).
Coronary Artery Calcium Score Predicts Major Adverse Cardiovascular Events in Stable Chest Pain
The DISCHARGE Trial Group
Radiology 2024; 310(3):e231557 - “In conclusion, in participants with stable chest pain referred for invasive coronary angiography, a coronary artery calcium score of 0 showed very low risk of major adverse cardiovascular events (MACE) at follow-up, and increasing scores were associated with increasing rates of obstructive coronary artery disease, revascularization, and MACE.”
Coronary Artery Calcium Score Predicts Major Adverse Cardiovascular Events in Stable Chest Pain
The DISCHARGE Trial Group
Radiology 2024; 310(3):e231557
Colon
- “GI bleeding can be characterized by the presumed location of origin. UGIB is defined as bleeding that originates from the esophagus, stomach, or duodenum. This accounts for approximately 80% of bleeding events. LGIB has previously been defined as bleeding that originates distal to the ligament of Treitz but more recently is defined as bleeding distal to the ileocecal valve and throughout the colon. LGIB, depending on its anatomic landmarks, accounts for approximately 15%–30% of all GI bleeding events. Finally, small bowel or midgut GI bleeding is defined as bleeding that occurs between the ligament of Treitz to the ileocecal valve and accounts for approximately 5%–10% of GI bleeding events.”
The Role of Imaging for GI Bleeding: ACG and SAR Consensus Recommendations.
Sengupta N,et al.
Radiology. 2024 Mar;310(3):e232298. doi: 10.1148/radiol.232298 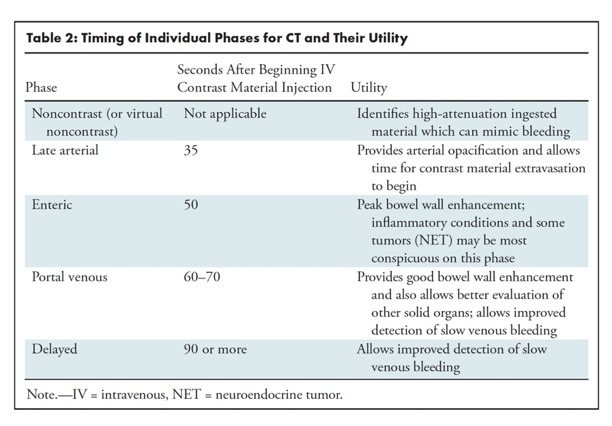
The Role of Imaging for GI Bleeding: ACG and SAR Consensus Recommendations.
Sengupta N,et al.
Radiology. 2024 Mar;310(3):e232298. doi: 10.1148/radiol.232298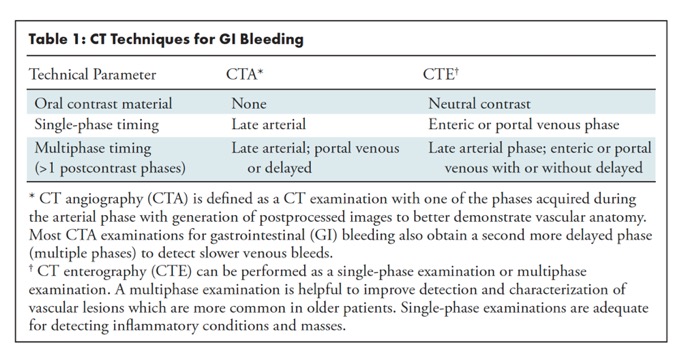
The Role of Imaging for GI Bleeding: ACG and SAR Consensus Recommendations.
Sengupta N,et al.
Radiology. 2024 Mar;310(3):e232298. doi: 10.1148/radiol.232298- “Because of its noninvasive nature, short examination time, and widespread availability, CTA is well-suited to evaluate patients with overt GI bleeding, particularly in hemodynamically unstable patients. In patients with overt GI bleeding, CT is used to identify intraluminal blood products or active contrast material extravasation to localize the site of hemorrhage and can also detect etiologies outside of the GI tract. CT techniques such as digital subtraction and dual-energy acquisition have improved the ability of CT to detect subtle GI tract lesions . CTA also provides additional information regarding the patient’s vascular and enteric anatomy, which is often helpful for choosing and planning a subsequent interventional radiology, endoscopic, or surgical procedure.”
The Role of Imaging for GI Bleeding: ACG and SAR Consensus Recommendations.
Sengupta N,et al.
Radiology. 2024 Mar;310(3):e232298. doi: 10.1148/radiol.232298 - “The biggest limitation of 99mTc-RBC scans is that this study can only be performed on hemodynamically stable patients. The RBC labeling preparation time and long imaging times prevents performing this study on patients who are hemodynamically unstable because of hypotension or abnormal heart rate. The risk-benefit ratio of obtaining a 99mTc-RBC scan, which has a long imaging time, versus correctly identifying an active LGIB site has to be weighed in borderline hemodynamically ,unstable patients.”
The Role of Imaging for GI Bleeding: ACG and SAR Consensus Recommendations.
Sengupta N,et al.
Radiology. 2024 Mar;310(3):e232298. doi: 10.1148/radiol.232298 - “CTE may have several advantages over endoscopic techniques. CTE has greater sensitivity for detecting small bowel masses, particularly those that are mural-based, and can help direct targeted, deep enteroscopy procedures when a source is identified. Cross-sectional imaging techniques (CT and MRI) allow visualization of extraintestinal abdominopelvic structures such as malignancies that may involve bowel or changes in the mesentery, bowel wall, and bowel/mesenteric vessels as potential causes of GI bleeding even in the absence of active contrast material extravasation. In patients with occult small bowel bleeding and relative contraindications to capsule endoscopy such as radiation, prior surgery, Crohn disease, and/or small bowel stenosis, CTE maybe the first-line study to characterize the abnormality .”
The Role of Imaging for GI Bleeding: ACG and SAR Consensus Recommendations.
Sengupta N,et al.
Radiology. 2024 Mar;310(3):e232298. doi: 10.1148/radiol.232298



Deep Learning
- “In summary, the ethical and effective deployment of AI in healthcare is substantially enhanced by rigorous QA protocols, transparent vendor practices, and a commitment to ongoing monitoring and adaptation. Through continuous monitoring and rigorous testing, QA ensures that medical AI tools remain reliable and effective across varied patient demographics and clinical scenarios. Rigorous testing procedures enhance their trustworthiness among clinicians and patients and support the broader goal of ensuring that AI tools can be effectively generalized to different settings. Integrating robust QA programs creates a more resilient healthcare system equipped to harness the benefits of AI while minimizing risks. These elements collectively contribute to making AI a more reliable, safe, and equitable tool in medicine, enabling healthcare providers to build trust and prevent harm while adapting to the evolving landscape of AI.”
Artificial intelligence in medicine: mitigating risks and maximizing benefits via quality assurance, quality control, and acceptance testing
Usman Mahmood Artificial intelligence in medicine: mitigating risks and maximizing benefits via quality assurance, quality control, and acceptance testing Usman Mahmood
BJR|Artificial Intelligence, 2024, 1(1), ubae003 - “Implementing AI tools into clinical practice is a shared responsibility between manufacturers and end-users2that should mirror the QA programs required to install medical imaging devices. The programs should include comprehensive acceptance testing (AT) and continued, periodic quality control (QC) procedures. End-user training and a proper trial period with the local patient population should be required to ensure an understanding of the intended use and limitations of the AI tools before the AI recommendation may influence clinical decisions. ”
Artificial intelligence in medicine: mitigating risks and maximizing benefits via quality assurance, quality control, and acceptance testing
Usman Mahmood Artificial intelligence in medicine: mitigating risks and maximizing benefits via quality assurance, quality control, and acceptance testing Usman Mahmood
BJR|Artificial Intelligence, 2024, 1(1), ubae003 - “Given the diverse applications of AI in medical imaging, each AI tool will require its own specific QA program. However, the general principle should be to assess each tool's functionality locally using well-curated, reference test sets with sufficient annotated cases for each subgroup in the local patient population. This approach involves evaluating the AI tool's performance across diverse patient subgroups that cover the local real-world patient population of interest, including subgroups that might be underrepresented in the initial training or pre-release test data. A carefully designed testing regime goes beyond mere accuracy metrics; it critically examines potential biases, sensitivity to specific anatomical variations, and the tool's adaptability to different clinical contexts. The increased scrutiny ensures that the AI tool operates equitably across a broader spectrum of patients, thereby building trust in its ability to generalize to the unique components of the local context. Additionally, the QA process should be tailored to the specific application, associated risks, and clinical environment in which it will be used.”
Artificial intelligence in medicine: mitigating risks and maximizing benefits via quality assurance, quality control, and acceptance testing
Usman Mahmood Artificial intelligence in medicine: mitigating risks and maximizing benefits via quality assurance, quality control, and acceptance testing Usman Mahmood
BJR|Artificial Intelligence, 2024, 1(1), ubae003 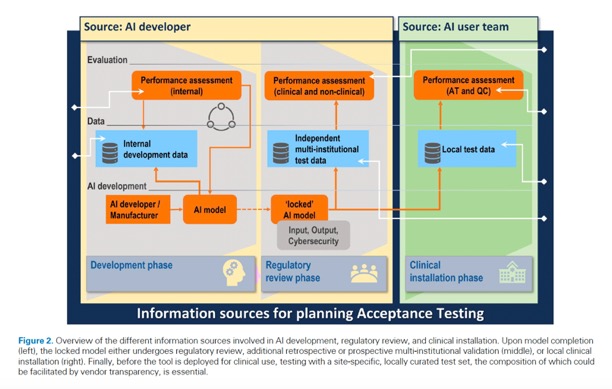
Artificial intelligence in medicine: mitigating risks and maximizing benefits via quality assurance, quality control, and acceptance testing
Usman Mahmood Artificial intelligence in medicine: mitigating risks and maximizing benefits via quality assurance, quality control, and acceptance testing Usman Mahmood
BJR|Artificial Intelligence, 2024, 1(1), ubae003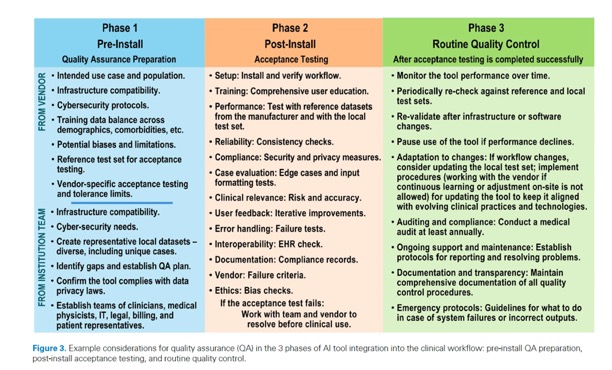
Artificial intelligence in medicine: mitigating risks and maximizing benefits via quality assurance, quality control, and acceptance testing
Usman Mahmood Artificial intelligence in medicine: mitigating risks and maximizing benefits via quality assurance, quality control, and acceptance testing Usman Mahmood
BJR|Artificial Intelligence, 2024, 1(1), ubae003- ”Building on the essential roles of AT and QC, user training is a critical element for successfully integrating AI tools into healthcare. To encourage adoption and minimize risks, the end-users must understand the tool’s intended use, capabilities, limitations, and ethical implications. Such training should be both comprehensive and tailored to meet the unique requirements and protocols of each clinical site.10-12 In addition to application-specific instructions, training modules should include information on the correct usage of the AI tool, underlying assumptions, legal framework, and case studies illustrating both successful and unsuccessful applications. This multifaceted approach aids in understanding the tool's strengths and limitations. Crucially, user training should commence before the AI tool starts influencing clinical decisions and should be periodically updated throughout the AI tool's operational life. Continuous education should include peer-reviewed audits and equip clinicians to effectively communicate the role and impact of AI tools in patient care. Furthermore, settings where AI outputs guide downstream decisions warrant additional discipline-specific training.”
Artificial intelligence in medicine: mitigating risks and maximizing benefits via quality assurance, quality control, and acceptance testing
Usman Mahmood Artificial intelligence in medicine: mitigating risks and maximizing benefits via quality assurance, quality control, and acceptance testing Usman Mahmood
BJR|Artificial Intelligence, 2024, 1(1), ubae003


- “Abdominal cancers continue to pose daily challenges to clinicians, radiologists and researchers. These challenges are faced at each stage of abdominal cancer management, including early detection, accurate characterization, precise assessment of tumor spread, preoperative planning when surgery is anticipated, prediction of tumor aggressiveness, response to therapy, and detection of recurrence. Technical advances in medical imaging, often in combination with imaging biomarkers, show great promise in addressing such challenges. Information extracted from imaging datasets owing to the application of radiomics can be used to further improve the diagnostic capabilities of imaging. However, the analysis of the huge amount of data provided by these advances is a difficult task in daily practice. Artificial intelligence has the potential to help radiologists in all these challenges. Notably, the applications of AI in the field of abdominal cancers are expanding and now include diverse approaches for cancer detection, diagnosis and classification, genomics and detection of genetic alterations, analysis of tumor microenvironment, identification of predictive biomarkers and follow-up. However, AI currently has some limitations that need further refinement for implementation in the clinical setting. This review article sums up recent advances in imaging of abdominal cancers in the field of image/data acquisition, tumor detection, tumor characterization, prognosis, and treatment response evaluation.”
CT and MRI of abdominal cancers: current trends and perspectives in the era of radiomics and artificial intelligence
Maxime Barat · Anna Pellat · Christine Hoeffel · Anthony Dohan · Romain Coriat · Elliot K. Fishman · Stéphanie Nougaret · Linda Chu · Philippe Soyer
Japanese Journal of Radiology (2024) 42:246–260 - “Technical advances in medical imaging, often in combination with imaging biomarkers, show great promise in addressing such challenges. Information extracted from imaging datasets owing to the application of radiomics can be used to further improve the diagnostic capabilities of imaging. However, the analysis of the huge amount of data provided by these advances is a difficult task in daily practice. Artificial intelligence has the potential to help radiologists in all these challenges. Notably, the applications of AI in the field of abdominal cancers are expanding and now include diverse approaches for cancer detection, diagnosis and classification, genomics and detection of genetic alterations, analysis of tumor microenvironment, identification of predictive biomarkers and follow-up. However, AI currently has some limitations that need further refinement for implementation in the clinical setting. This review article sums up recent advances in imaging of abdominal cancers in the field of image/data acquisition, tumor detection, tumor characterization, prognosis, and treatment response evaluation.”
CT and MRI of abdominal cancers: current trends and perspectives in the era of radiomics and artificial intelligence
Maxime Barat · Anna Pellat · Christine Hoeffel · Anthony Dohan · Romain Coriat · Elliot K. Fishman · Stéphanie Nougaret · Linda Chu · Philippe Soyer
Japanese Journal of Radiology (2024) 42:246–260 - “Radiomics can be used for several tasks such as characterizing indeterminate liver lesions in patients with cirrhosis or pancreatic tumors, grading HCC or pancreatic neuroendocrine tumors (pNETs) , identifying microvascular invasion (MVI) in HCC (TACE) or transarterial radioembolization. More recently, radiomics has demonstrated utility for the assessment of tumor microenvironment, which is a relatively new concept that refers to an assemblage of multiple elements contained in tissues that surround tumor. Tumor microenvironment is a dynamic and heterogeneous assemblage made of precursor cells, fibroblasts, immune cells, endothelial cells, signaling molecules, and extracellular matrix components that play a major role in cancer biology. Tumor microenvironment is involved in tumor growth, invasion, metastasis but also in response or resistance to systemic therapies and local therapies such as thermal ablation.”
CT and MRI of abdominal cancers: current trends and perspectives in the era of radiomics and artificial intelligence
Maxime Barat · Anna Pellat · Christine Hoeffel · Anthony Dohan · Romain Coriat · Elliot K. Fishman · Stéphanie Nougaret · Linda Chu · Philippe Soyer
Japanese Journal of Radiology (2024) 42:246–260 - “Radiomics models have been developed to predict response to local intra-arterial therapy of HCC. Park et al. found that HCCs with complete response after TACE show lower homogeneity at CT-texture analysis than those with partial response. A hybrid model combining CT-based radiomic features and three clinical factors (Child–Pugh score, a-fetoprotein level, and HCC size) was a strong predictor of longer survival in patients with HCC treated using TACE (hazard ratio 19.88; 95% CI 6.37–62.02) (p < 0.0001). Interestingly, in a study by Aujay et al., MRI based radiomics outperformed RECIST criteria and Liver Imaging Reporting and Data System treatment response algorithm for the assessment of early response of locally advanced HCC to 90yttrium transarterial radioembolization.”
CT and MRI of abdominal cancers: current trends and perspectives in the era of radiomics and artificial intelligence
Maxime Barat · Anna Pellat · Christine Hoeffel · Anthony Dohan · Romain Coriat · Elliot K. Fishman · Stéphanie Nougaret · Linda Chu · Philippe Soyer
Japanese Journal of Radiology (2024) 42:246–260 - “Owing to the development of radiomics, CT and MRI can now be used as predictive tools to better estimate response to treatment. Although major advances have been made in abdominal cancer imaging with promising results, these results are still at an early stage and often obtained with local algorithms. Although AI helps extract a huge number of features and classify them, there is a need to bring together all the information to use it in a more efficient way. The next step should be to investigate how all these advances can be implemented in the real-life setting and how they can positively influence care and outcomes in patients with abdominal cancers .State of the art imaging is forcing radiologists to rethink what they do and how they should do it. Current challenges to implementation include reimbursement issues and well-designed translational trials for AI validation that need large volumes of high-quality and representative data for the development of robust AI algorithms.”
CT and MRI of abdominal cancers: current trends and perspectives in the era of radiomics and artificial intelligence
Maxime Barat · Anna Pellat · Christine Hoeffel · Anthony Dohan · Romain Coriat · Elliot K. Fishman · Stéphanie Nougaret · Linda Chu · Philippe Soyer
Japanese Journal of Radiology (2024) 42:246–260 - Rationale and objectives: Automated evaluation of abdominal computed tomography (CT) scans should help radiologists manage their massive workloads, thereby leading to earlier diagnoses and better patient outcomes. Our objective was to develop a machine-learning model capable of reliably identifying suspected bowel obstruction (BO) on abdominal CT.
Conclusion: The 3D mixed convolutional neural network developed here shows great potential for the automated binary classification (BO yes/no) of abdominal CT scans from patients with suspected BO.
Clinical relevance statement: The 3D mixed CNN automates bowel obstruction classification, potentially automating patient selection and CT prioritization, leading to an enhanced radiologist workflow.
Deep learning for automatic bowel-obstruction identification on abdominal CT
Quentin Vanderbecq et al.
European Radiology https://doi.org/10.1007/s00330-024-10657 - Key Points
• Bowel obstruction’s rising incidence strains radiologists. AI can aid urgent CT readings.
• Employed 1345 CT scans, neural networks for bowel obstruction detection, achieving high accuracy and sensitivity on external testing.
• 3D mixed CNN automates CT reading prioritization effectively and speeds up bowel obstruction diagnosis.
Deep learning for automatic bowel-obstruction identification on abdominal CT
Quentin Vanderbecq et al.
European Radiology https://doi.org/10.1007/s00330-024-10657
Improving Efficiencies While Also Delivering Better Health Care Outcomes: A Role for Large Language Models.
Rao SK, Fishman EK, Rizk RC, Chu LC, Rowe SP.
J Am Coll Radiol. 2024 Jan 12:S1546-1440(24)00005-X. doi: 10.1016/j.jacr.2024.01.003. Epub ahead of print. PMID: 38220038.- “Generative artificial intelligence (AI), specifically the large language models (LLMs) that underlie impressive new applications such as ChatGPT, are already fundamentally changing medicine. Unlike more traditional AI systems that produce simple outputs such as a number (say, the predicted length of stay for a patient in the hospital) or a category (say, “malignant” or “benign” for a radiologic system), “generative AI” refers broadly to systems whose outputs take the form of more unstructured media objects, such as images and documents. Under the hood, many of these systems are actually built by executing models that serve a more classical purpose. Generative text models, for example, generate whole documents by iteratively predicting “what word comes next.” But the ability to produce a whole document with desired properties unlocks a host of exciting applications.”
Improving Efficiencies While Also Delivering Better Health Care Outcomes: A Role for Large Language Models.
Rao SK, Fishman EK, Rizk RC, Chu LC, Rowe SP.
J Am Coll Radiol. 2024 Jan 12:S1546-1440(24)00005-X. doi: 10.1016/j.jacr.2024.01.003. Epub ahead of print. PMID: 38220038 - “We build and leverage generative AI to unburden clinicians from clerical work to help them focus more fully on their patients. Briefly, Abridge AI helps clinicians capture conversations, structure and summarize the information exchanged, and integrate that information back into the medical record. As clinicians, we are tasked to serve three constituents for patients we see. Those constituents are (1) our care team members, who benefit from clinical notes that convey our thought process; (2) ourselves, as the physicians who also need to place orders, report diagnostic codes, and handle procedure codes for billing and revenue cycle; and (3) our patients, the most important constituents, who benefit from visit summaries and access to their OpenNotes in their portals.”
Improving Efficiencies While Also Delivering Better Health Care Outcomes: A Role for Large Language Models.
Rao SK, Fishman EK, Rizk RC, Chu LC, Rowe SP.
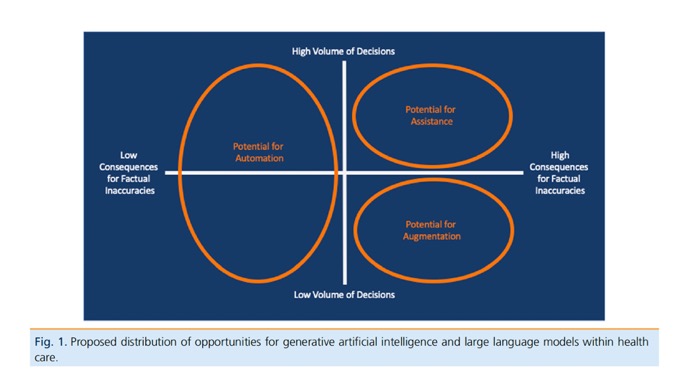
J Am Coll Radiol. 2024 Jan 12:S1546-1440(24)00005-X. doi: 10.1016/j.jacr.2024.01.003. Epub ahead of print. PMID: 38220038 - “The arrival of LLMs that can provide real-time assistance to physicians may allow a remarkable increase in their bandwidth, regardless of specialty. In radiology, leveraging these emerging technologies will potentially allow more scans to be read without adding burden or stress to the interpreting radiologist. We would be in the “high consequences for factual inaccuracies and high volume of decisions” quadrant of Figure 1, where the assistance of an LLM would be its key feature. The importance of that added bandwidth would be its potential to ameliorate disparities by democratizing the expertise of radiologists who are already able to handle large volumes or who may have special skill sets in less common examinations. Such improvements in access to care would hopefully have downstream effects of improved outcomes in marginalized populations.”
Improving Efficiencies While Also Delivering Better Health Care Outcomes: A Role for Large Language Models.
Rao SK, Fishman EK, Rizk RC, Chu LC, Rowe SP.
J Am Coll Radiol. 2024 Jan 12:S1546-1440(24)00005-X. doi: 10.1016/j.jacr.2024.01.003. Epub ahead of print. PMID: 38220038

Kidney
- Purpose: To investigate the prevalence of FLCN, BAP1, SDH, and MET mutations in an oncologic cohort and determine the prevalence, clinical features, and imaging features of renal cell carcinoma (RCC) associated with these mutations. Secondarily, to determine the prevalence of encountered benign renal lesions.
Materials and Methods: From 25 220 patients with cancer who prospectively underwent germline analysis with a panel of more than 70 cancer-predisposing genes from 2015 to 2021, patients with FLCN, BAP1, SDH, or MET mutations were retrospectively identified. Clinical records were reviewed for patient age, sex, race/ethnicity, and renal cancer diagnosis. If RCC was present, baseline CT and MRI examinations were independently assessed by two radiologists. Summary statistics were used to summarize continuous and categorical variables by mutation.
Conclusion: FLCN, BAP1, SDH, and MET mutations were present in less than 1% of this oncologic cohort. Within the study sample size limits, imaging findings for hereditary RCC overlapped with those of nonhereditary RCC, and the prevalence of other associated benign solid renal lesions (other than complex cysts) was up to 11%.
The Prevalence and Radiologic Features of Renal Cancers Associated with FLCN, BAP1, SDH, and MET Germline Mutations
Charlotte Charbel, MD et al.
Radiology: Imaging Cancer 2024; 6(2):e230063 - Key Points
■ FLCN, BAP1, SDH, and MET germline mutations were present in less than 1% of an oncologic cohort of more than 25 000 patients.
■ The most prevalent renal cell carcinoma (RCC) histologic subtype for FLCN, BAP1, SDH, and MET mutations was unclassified RCC (three of four, 75%), clear cell RCC (three of four, 75%), SDH-deficient RCC (six of nine, 67%), and papillary RCC (one of one, 100%), respectively.
■ The radiologic features of hereditary RCC at CT and MRI in the 18 patients diagnosed with RCC overlapped with those of patients with nonhereditary RCC, and the prevalence of encountered benign renal lesions was up to 11% for oncocytomas and angiomyolipomas.
The Prevalence and Radiologic Features of Renal Cancers Associated with FLCN, BAP1, SDH, and MET Germline Mutations
Charlotte Charbel, MD et al.
Radiology: Imaging Cancer 2024; 6(2):e230063 - Hereditary renal cell carcinoma (RCC) accounts for 5%– 8% of all malignant renal tumors (1). To date, the National Comprehensive Cancer Network recognizes seven hereditary RCC syndromes (with their respective mutated genes): Von Hippel–Lindau syndrome (VHL), Birt-Hogg- Dubé syndrome (FLCN), tuberous sclerosis complex (TSC1-2), hereditary leiomyomatosis and RCC (FH), BAP1 tumor predisposition syndrome (BAP1), hereditary paraganglioma/pheochromocytoma syndrome (SDHAF2, SDHB, SDHC, and SDHD, henceforth together referred to as SDH), and hereditary papillary renal carcinoma (MET).
The Prevalence and Radiologic Features of Renal Cancers Associated with FLCN, BAP1, SDH, and MET Germline Mutations
Charlotte Charbel, MD et al.
Radiology: Imaging Cancer 2024; 6(2):e230063 - “The radiologic features of RCC associated with FLCN, BAP1, SDH, and MET mutations in our oncologic cohort were similar to those of sporadic RCC, with most tumors demonstrating ill-defined margins, heterogeneous enhancement, and internal necrotic/cystic components. Tumors also had the potential to invade the renal sinus (BAP1, FLCN, and SDH mutations), hilar collecting system (BAP1, SDH, and FLCN mutations), and renal vein (BAP1 and FLCN mutations). None of the hereditary RCC syndromes were associated with additional imaging features distinguishing hereditary RCC from sporadic RCC.”
The Prevalence and Radiologic Features of Renal Cancers Associated with FLCN, BAP1, SDH, and MET Germline Mutations
Charlotte Charbel, MD et al.
Radiology: Imaging Cancer 2024; 6(2):e230063 - “In conclusion, the prevalence of FLCN, BAP1, SDH, and MET mutations was less than 1%, even in an oncologic cohort. These mutations should be suspected if RCC is present in younger patients, patients with RCC and other cancers or fibrofolliculomas or lung cysts, or patients with multifocal RCC. Nevertheless, with our sample size, we found no distinct radiologic features of hereditary renal cell carcinoma or significant association with other benign renal lesions.”
The Prevalence and Radiologic Features of Renal Cancers Associated with FLCN, BAP1, SDH, and MET Germline Mutations
Charlotte Charbel, MD et al.
Radiology: Imaging Cancer 2024; 6(2):e230063
Pancreas
- “Abdominal cancers continue to pose daily challenges to clinicians, radiologists and researchers. These challenges are faced at each stage of abdominal cancer management, including early detection, accurate characterization, precise assessment of tumor spread, preoperative planning when surgery is anticipated, prediction of tumor aggressiveness, response to therapy, and detection of recurrence. Technical advances in medical imaging, often in combination with imaging biomarkers, show great promise in addressing such challenges. Information extracted from imaging datasets owing to the application of radiomics can be used to further improve the diagnostic capabilities of imaging. However, the analysis of the huge amount of data provided by these advances is a difficult task in daily practice. Artificial intelligence has the potential to help radiologists in all these challenges. Notably, the applications of AI in the field of abdominal cancers are expanding and now include diverse approaches for cancer detection, diagnosis and classification, genomics and detection of genetic alterations, analysis of tumor microenvironment, identification of predictive biomarkers and follow-up. However, AI currently has some limitations that need further refinement for implementation in the clinical setting. This review article sums up recent advances in imaging of abdominal cancers in the field of image/data acquisition, tumor detection, tumor characterization, prognosis, and treatment response evaluation.”
CT and MRI of abdominal cancers: current trends and perspectives in the era of radiomics and artificial intelligence
Maxime Barat · Anna Pellat · Christine Hoeffel · Anthony Dohan · Romain Coriat · Elliot K. Fishman · Stéphanie Nougaret · Linda Chu · Philippe Soyer
Japanese Journal of Radiology (2024) 42:246–260 - “Technical advances in medical imaging, often in combination with imaging biomarkers, show great promise in addressing such challenges. Information extracted from imaging datasets owing to the application of radiomics can be used to further improve the diagnostic capabilities of imaging. However, the analysis of the huge amount of data provided by these advances is a difficult task in daily practice. Artificial intelligence has the potential to help radiologists in all these challenges. Notably, the applications of AI in the field of abdominal cancers are expanding and now include diverse approaches for cancer detection, diagnosis and classification, genomics and detection of genetic alterations, analysis of tumor microenvironment, identification of predictive biomarkers and follow-up. However, AI currently has some limitations that need further refinement for implementation in the clinical setting. This review article sums up recent advances in imaging of abdominal cancers in the field of image/data acquisition, tumor detection, tumor characterization, prognosis, and treatment response evaluation.”
CT and MRI of abdominal cancers: current trends and perspectives in the era of radiomics and artificial intelligence
Maxime Barat · Anna Pellat · Christine Hoeffel · Anthony Dohan · Romain Coriat · Elliot K. Fishman · Stéphanie Nougaret · Linda Chu · Philippe Soyer
Japanese Journal of Radiology (2024) 42:246–260 - “Radiomics can be used for several tasks such as characterizing indeterminate liver lesions in patients with cirrhosis or pancreatic tumors, grading HCC or pancreatic neuroendocrine tumors (pNETs) , identifying microvascular invasion (MVI) in HCC (TACE) or transarterial radioembolization. More recently, radiomics has demonstrated utility for the assessment of tumor microenvironment, which is a relatively new concept that refers to an assemblage of multiple elements contained in tissues that surround tumor. Tumor microenvironment is a dynamic and heterogeneous assemblage made of precursor cells, fibroblasts, immune cells, endothelial cells, signaling molecules, and extracellular matrix components that play a major role in cancer biology. Tumor microenvironment is involved in tumor growth, invasion, metastasis but also in response or resistance to systemic therapies and local therapies such as thermal ablation.”
CT and MRI of abdominal cancers: current trends and perspectives in the era of radiomics and artificial intelligence
Maxime Barat · Anna Pellat · Christine Hoeffel · Anthony Dohan · Romain Coriat · Elliot K. Fishman · Stéphanie Nougaret · Linda Chu · Philippe Soyer
Japanese Journal of Radiology (2024) 42:246–260 - “Radiomics models have been developed to predict response to local intra-arterial therapy of HCC. Park et al. found that HCCs with complete response after TACE show lower homogeneity at CT-texture analysis than those with partial response. A hybrid model combining CT-based radiomic features and three clinical factors (Child–Pugh score, a-fetoprotein level, and HCC size) was a strong predictor of longer survival in patients with HCC treated using TACE (hazard ratio 19.88; 95% CI 6.37–62.02) (p < 0.0001). Interestingly, in a study by Aujay et al., MRI based radiomics outperformed RECIST criteria and Liver Imaging Reporting and Data System treatment response algorithm for the assessment of early response of locally advanced HCC to 90yttrium transarterial radioembolization.”
CT and MRI of abdominal cancers: current trends and perspectives in the era of radiomics and artificial intelligence
Maxime Barat · Anna Pellat · Christine Hoeffel · Anthony Dohan · Romain Coriat · Elliot K. Fishman · Stéphanie Nougaret · Linda Chu · Philippe Soyer
Japanese Journal of Radiology (2024) 42:246–260 - “Owing to the development of radiomics, CT and MRI can now be used as predictive tools to better estimate response to treatment. Although major advances have been made in abdominal cancer imaging with promising results, these results are still at an early stage and often obtained with local algorithms. Although AI helps extract a huge number of features and classify them, there is a need to bring together all the information to use it in a more efficient way. The next step should be to investigate how all these advances can be implemented in the real-life setting and how they can positively influence care and outcomes in patients with abdominal cancers .State of the art imaging is forcing radiologists to rethink what they do and how they should do it. Current challenges to implementation include reimbursement issues and well-designed translational trials for AI validation that need large volumes of high-quality and representative data for the development of robust AI algorithms.”
CT and MRI of abdominal cancers: current trends and perspectives in the era of radiomics and artificial intelligence
Maxime Barat · Anna Pellat · Christine Hoeffel · Anthony Dohan · Romain Coriat · Elliot K. Fishman · Stéphanie Nougaret · Linda Chu · Philippe Soyer
Japanese Journal of Radiology (2024) 42:246–260
- Purpose: Accurate staging of disease is vital in determining appropriate care for patients with pancreatic ductal adenocarcinoma (PDAC). It has been shown that the quality of scans and the experience of a radiologist can impact computed tomography (CT) based assessment of disease. The aim of the current study was to evaluate the impact of the rereading of outside hospital (OH) CT by an expert radiologist and a repeat pancreatic protocol CT (PPCT) on staging of disease.
Conclusion: A repeat PPCT results in increased detection of metastatic disease that rereviews of OH scans may otherwise miss. Accessible insurance coverage for repeat PPCT imaging even within 30 days of an OH scan could help optimize delivery of care and alleviate burdens associated with misstaging.
Factors associated with radiological misstaging of pancreatic ductal adenocarcinoma: A retrospective observational study.
Yasrab M, Thakker S, Wright MJ, Ahmed T, He J, Wolfgang CL, Chu LC, Weiss MJ, Kawamoto S, Johnson PT, Fishman EK, Javed AA
Curr Probl Diagn Radiol. 2024 Mar 7:S0363-0188(24)00047-1. doi: 10.1067/j.cpradiol.2024.03.001. Epub ahead of print. PMID: 38522966. - “Pancreatic imaging, however, has its pitfalls and challenges, which are driven in part by the type and quality of the scanners, expertise of the technologists, and the experience of the radiologists interpreting these images.11 Misstaging of disease has clinical implications for patient care; for instance, in the event of undetected metastases, surgical resection is aborted intraoperatively. The current rate of occult metastatic disease has been estimated to range from 8 % to 24.5 %.”
Factors associated with radiological misstaging of pancreatic ductal adenocarcinoma: A retrospective observational study.
Yasrab M, Thakker S, Wright MJ, Ahmed T, He J, Wolfgang CL, Chu LC, Weiss MJ, Kawamoto S, Johnson PT, Fishman EK, Javed AA
Curr Probl Diagn Radiol. 2024 Mar 7:S0363-0188(24)00047-1. doi: 10.1067/j.cpradiol.2024.03.001. Epub ahead of print. PMID: 38522966. - “Rereading an OH scan by an experienced radiologist caught previously missed metastatic disease in 21.5 % (11/51) of those who were misstaged. When the OH scan was compared directly to a PPCT, it resulted in the most prominent change in terms of absolute numbers (70/100) with 35.7 % (25/70) cases of missed metastatic disease. While rereviewing an OH scan results in led to a higher total number of misstaged cases, it still did not fully capture the absolute number of patients with occult metastatic disease that a repeat PPCT detected. This is showcased when comparing the OH scan rereviews to the PPCT, which reveals that missed metastases comprise the bulk of misstaged cases 62.5 % (15/24) that a reread did not pick up.”
Factors associated with radiological misstaging of pancreatic ductal adenocarcinoma: A retrospective observational study.
Yasrab M, Thakker S, Wright MJ, Ahmed T, He J, Wolfgang CL, Chu LC, Weiss MJ, Kawamoto S, Johnson PT, Fishman EK, Javed AA
Curr Probl Diagn Radiol. 2024 Mar 7:S0363-0188(24)00047-1. doi: 10.1067/j.cpradiol.2024.03.001. Epub ahead of print. PMID: 38522966. - “In conclusion, this study redemonstrates the need for adherence to protocols for PPCT when assessing patients with PDAC. Furthermore, in the event of a suboptimal scan, a repeat PPCT is warranted, even if performed within 30 days of a prior scan, given the risk of missing metastatic disease. Increased utilization of PPCT, standardized templates, expert radiologist rereads, and insurance coverage for reimaging could help alleviate the psychological and financial burdens associated with misstaging of disease on both the patients and the healthcare system. ”
Factors associated with radiological misstaging of pancreatic ductal adenocarcinoma: A retrospective observational study.
Yasrab M, Thakker S, Wright MJ, Ahmed T, He J, Wolfgang CL, Chu LC, Weiss MJ, Kawamoto S, Johnson PT, Fishman EK, Javed AA
Curr Probl Diagn Radiol. 2024 Mar 7:S0363-0188(24)00047-1. doi: 10.1067/j.cpradiol.2024.03.001. Epub ahead of print. PMID: 38522966.
- “Pancreatic neuroendocrine tumours (PNETs) are a rare subset of pancreatic tumours that have historically comprised up to 3% of all clinically detected pancreatic tumours. In recent decades, however, advancements in imaging have led to an increased incidental detection rate of PNETs and imaging has played an increasingly central role in the initial diagnostics and surgical planning of these tumours. Cinematic rendering (CR) is a 3D post-processing technique that generates highly photorealistic images through more realistically modelling the path of photons through the imaged volume. This allows for more comprehensive visualization, description, and interpretation of anatomical structures. In this 2-part review article, we present the first description of the various CR appearances of PNETs in the reported literature while providing commentary on the unique clinical opportunities afforded by the adjunctive utilization of CR in the workup of these rare tumours.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 1: Tumour Detection and Characterization
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - At CT, PNETs typically appear as well circumscribed avidly enhancing masses that may arise from any portion of the pancreas. Enhancement patterns for small PNETs are usually uniform, and some may present with a characteristic rim enhancement that can help clue in the diagnosis. The degree and homogeneity of lesion enhancement is correlated with tumour grade, and among larger PNETs, which predominantly consist of non-hyperfunctioning variants, the presence of cystic degeneration, intralesional necrosis and calcification can result in an inhomogeneous pattern of enhancement. PNETs are classically best visualized in the arterial phase. While smaller PNETs can be particularly difficult to see on venous or delayed images, a small proportion of PNETs may atypically be better visualized on portal venous phase imaging.
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 1: Tumour Detection and Characterization
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - Differential diagnoses of PNETs consist of pancreatic metastases, most often from renal cell carcinoma, solid variant serous cystadenoma, peripancreatic gastrointestinal stromal tumour, and intrapancreatic accessory spleen.5 In rarer cases of hypovascular PNETs, differentiation from adenocarcinoma is essential and carries significant implications for management.
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 1: Tumour Detection and Characterization
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - “Cinematic rendering may allow for the detection of the presence of tumour in cases where subtle textural changes due to inherent differences between normal and abnormal tissue are present, but a defined mass is not yet visible. Through this, CR can potentially facilitate early disease detection and help differentiate PNETs from normal pancreatic parenchyma. CR can similarly assist in differentiating PNETs from intrapancreatic accessory spleens through accentuating textural differences that may not be appreciable at non-cinematic imaging . Display configurations of CR may also be manipulated to conceal uninvolved pancreatic parenchyma, allowing for isolated visualization of PNETs. This can make tumours remarkably conspicuous as well as highlight the spatial relationship of the tumour with extra-pancreatic anatomy.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 1: Tumour Detection and Characterization
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - “While PNETs are typically solid tumours, the presence of cystic internal components is not uncommon, with up to 10% of PNETs being purely cystic. Cystic components in PNETs are most often encountered among larger PNETs that undergo cystic degeneration or necrosis. Rarely, small PNETs with cystic change are also encountered and can pose diagnostic challenges. Purely cystic PNETs generally exhibit more indolent behaviour and carry more favourable prognoses, which has also led to the rise of conflicting opinions regarding the value of resection in these cases.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 1: Tumour Detection and Characterization
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - “Purely cystic PNETs generally exhibit more indolent behaviour and carry more favourable prognoses, which has also led to the rise of conflicting opinions regarding the value of resection in these cases.19 Simultaneously however, cystic PNET can be misdiagnosed as a potentially malignant cystic lesion (ie, mucinous cystic neoplasm, intraductal papillary neoplasm) that ought to be resected, or a benign cystic lesion (ie, serous cystadenoma) for which surgery is not indicated, which can lead to suboptimal patient outcomes. Radiological characterization of the internal architecture of these tumours is therefore particularly important due to the wide range of potential implications upon management.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 1: Tumour Detection and Characterization
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705.. - “Cinematic rendering is uniquely suited to visualization of these cases through its ability to greatly improve depth perception. Improved depth perception, in conjunction with dynamic textural visualization of CR may allow for optimal characterization of the internal architecture of cystic components. This can result in superior visualization of fine internal septations and mural nodularity within these lesions that may help in differentiating them from other cystic pancreatic lesions. In particular, the presence of an avidly enhancing hypervascular rim, owing to the rich blood supply of PNETs, is known to be a highly suggestive radiologic feature of cystic PNETs. Improved characterization of the cystic mural interface using CR may be especially advantageous in appreciating this key finding.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 1: Tumour Detection and Characterization
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. 
- “Precise evaluation of the presence and extent of vascular invasion is essential in determining the resectability of PNETs and to plan for possible vascular reconstruction. Though CT is considered to have excellent sensitivity in identifying major vessel involvement, prior studies have found that 25% to 50% of patients with PNETs who are radiologically determined to have vascular invasion, are confirmed to have true vascular invasion at the time of surgery. On the more concerning flipside of this, it is similarly possible that patients with softer radiological signs of vascular invasion may be denied surgery due to perceived vascular involvement in the absence of true involvement. In these equivocal cases, vascular abutment may be misinterpreted as vascular encasement and vice versa. CR may alleviate the diagnostic burden in these cases by generating exquisitely detailed vascular maps that allow radiologists to visualize the tumour-vessel interface with increased confidence. Through this, it may be possible to differentiate vascular stretching, abutment, and compression from true vessel invasion. Radiological assessment of vascular involvement in PNETs is also uniquely nuanced as PNETs may not traditionally encase vessels but instead tend to invade and expand venous vasculature.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 2: Preoperative Planning and Evaluation of Metastatic Disease.
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - “Unlike PDAC, the presence of hepatic metastases in PNETs does not preclude surgical resection, and potentially curative resection of the primary tumour and metastatic hepatic implants is still possible in up to 25% of patients.14 Timely radiological identification of hepatic metastases and subsequent deliberation of their resectability is therefore critical to the management of metastatic PNETs. Using CR, rendering parameters can be modified to either highlight the characteristically hypervascular metastases but may also be adjusted to optimize visualization in cases of atypical hypovascular-appearing metastases. Display settings can also be further modified to render the background hepatic parenchyma translucent to further accentuate any hepatic metastases. Once lesions are identified, the enhanced depth perception of CR can also help differentiate them from benign liver lesions through improving visualization of their internal architecture. “
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 2: Preoperative Planning and Evaluation of Metastatic Disease.
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - “CR augmentation also has the potential to go beyond optimizing disease detection and classification and may also impact surgical planning. This is achieved through the generation of photorealistic images that essentially serve as personalized anatomic models for the operating team. Anecdotally, pancreatic surgeons at our institution have found these reconstructions helpful for preoperative planning and in improving intraoperative situational awareness. This is particularly relevant in cases of laparoscopic surgery, where real-time intraoperative visualization is restricted.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 2: Preoperative Planning and Evaluation of Metastatic Disease.
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - “While CR has shown promise in enhancing the diagnostics and surgical planning of PNETs in our institution, there remain certain limitations that hinder broader adoption. One significant constraint revolves around the specialized expertise required to generate CR images. Optimization of CR images is crucial to accurately represent the anatomy and pathology of interest. This task demands the dedicated training of radiologists who need to customize the display settings for each specific pathology. Using incorrect parameters can impede visualization and may result in incorrect diagnoses. This is compounded by the shadowing effects generated by the CR global lighting model which if not duly accounted for may potentially obscure visualization of significant pathology. As CR becomes more widely adopted, this aspect of CR is anticipated to become more standardized and perhaps even automated.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 2: Preoperative Planning and Evaluation of Metastatic Disease.
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705. - “CR holds promising potential for enhancing the diagnostics and surgical planning of PNETs. Part 2 of this pictorial review highlights the utility of CR in vascular mapping, preoperative planning, and evaluation of metastatic disease of PNETs. In the words of Dr. O’Brien, cinematic rendering, though still in its infancy, is an exciting technique; future studies investigating implementation of CR into clinical practice have potential to add great value to our practice.”
Cinematic Rendering of Pancreatic Neuroendocrine Tumours: Opportunities for Clinical Implementation: Part 2: Preoperative Planning and Evaluation of Metastatic Disease.
Ahmed TM, Fishman EK, Chu LC.
Can Assoc Radiol J. 2024 Mar 20:8465371241239035. Epub ahead of print. PMID: 38509705.


- The radiologic finding of focal stenosis of the main pancreatic duct is highly suggestive of pancreatic cancer. Even in the absence of a mass lesion, focal duct stenosis can lead to surgical resection of the affected portion of the pancreas. We present four patients with distinctive pathology associated with non-neoplastic focal stenosis of the main pancreatic duct. The pathology included stenosis of the pancreatic duct accompanied by wavy, acellular, serpentine-like fibrosis, chronic inflammation with foreign body–type giant cell reaction, and calcifications. In all cases, the pancreas toward the tail of the gland had obstructive changes including acinar drop-out and interlobular and intralobular fibrosis. Three of the four patients had a remote history of major motor vehicle accidents associated with severe abdominal trauma. These results emphasize that blunt trauma can injure the pancreas and that this injury can result in long term complications, including focal stenosis of the main pancreatic duct. Pathologists should be aware of the distinct pathology associated with remote trauma and, when the pathology is present, should elicit the appropriate clinical history.
Distinctive Pathology Associated With Focal Stenosis of the Main Pancreatic Duct Secondary to Remote Trauma: A Long-term Complication of Seat Belt Pancreatitis.
Wu AA, Thompson ED, Cameron JL, He J, Burkhart RA, Burns WR, Lafaro KJ, Shubert CR, Canto MI, Fishman EK, Hruban RH.
Am J Surg Pathol. 2024 Mar 14. doi: 10.1097/PAS.0000000000002207. Epub ahead of print. PMID: 38482693. - “Four cases of non-neoplastic cutoff of the main pancreatic duct with distinctive pathology are presented. The pathology included abrupt duct stenosis, changes suggestive of rupture of the pancreatic duct, wavy, acellular, serpentine-like stromal fibrosis, and a foreign body– type giant cell reaction. IgG4 immunohistochemical stain was below the threshold in all cases, ruling out a type 1 autoimmune pancreatitis, and no neoplasms were present. Three of the four patients had a history of major motor vehicle accidents with associated severe abdominal trauma, suggesting that the unique pathology was caused by the trauma.”
Distinctive Pathology Associated With Focal Stenosis of the Main Pancreatic Duct Secondary to Remote Trauma : A Long-term Complication of Seat Belt Pancreatitis
Annie A. Wu, MD, PhD,* Elizabeth D. Thompson, MD, PhD,*† John L. Cameron, MD,‡ Jin He, MD, PhD,‡ Richard A. Burkhart, MD,‡ William R. Burns, MD,‡ Kelly J. Lafaro, MD, MPH,‡ Christopher R. Shubert, MD, MHA,‡ Marcia I. Canto, MD, MHS,†§ Elliot K. Fishman, MD,∥ and Ralph H. Hruban, MD*†
Am J Surg Pathol 2024;00:000–000) (in press) 

Practice Management
- “The degree of intra-individual or personal variation was from 3 to 31 per cent. This degree of variation was surprising to many, even to persons whose scientific training and background should have led them to anticipate it, in view of the known element of error in all fields.”
On the Scientific Evaluation of Diagnostic Procedures
L. Henry Garland
Radiology Vol. S2 March 1949 No. 3; page 309-328 - “The degree of inter-individual variation, based only on the positives and not on all cases read, was from 9 to 24 per cent. This variation included cases of extensive disease, and was not due to the fact that only small or difficult lesions were being analyzed. Variation can be measured in different ways. As an example, if in a set of 100 films there are 4 positive and 96 negative films and a reader selects only 2 of the positive, and calls the remaining 98 negative, he might be regarded, by one standard, as being only 2 per cent wrong or inconsistent. On the other hand, if the set of films consists of survey material, the object of which is to detect all the positives, he might be regarded as 50 per cent wrong. In the percentages recorded in these paragraphs, the second criterion is being used.”
On the Scientific Evaluation of Diagnostic Procedures
L. Henry Garland
Radiology Vol. S2 March 1949 No. 3; page 309-328 - “The degree of inter-individual variation, based only on the positives and not on all cases read, was from 9 to 24 per cent. This variation included cases of extensive disease, and was not due to the fact that only small or difficult lesions were being analyzed. Variation can be measured in different ways. As an example, if in a set of 100 films there are 4 positive and 96 negative films and a reader selects only 2 of the positive, and calls the remaining 98 negative, he might be regarded, by one standard, as being only 2 per cent wrong or inconsistent. On the other hand, if the set of films consists of survey material, the object of which is to detect all the positives, he might be regarded as 50 per cent wrong.”
On the Scientific Evaluation of Diagnostic Procedures
L. Henry Garland
Radiology Vol. S2 March 1949 No. 3; page 309-328
Small Bowel
- “GI bleeding can be characterized by the presumed location of origin. UGIB is defined as bleeding that originates from the esophagus, stomach, or duodenum. This accounts for approximately 80% of bleeding events. LGIB has previously been defined as bleeding that originates distal to the ligament of Treitz but more recently is defined as bleeding distal to the ileocecal valve and throughout the colon. LGIB, depending on its anatomic landmarks, accounts for approximately 15%–30% of all GI bleeding events. Finally, small bowel or midgut GI bleeding is defined as bleeding that occurs between the ligament of Treitz to the ileocecal valve and accounts for approximately 5%–10% of GI bleeding events.”
The Role of Imaging for GI Bleeding: ACG and SAR Consensus Recommendations.
Sengupta N,et al.
Radiology. 2024 Mar;310(3):e232298. doi: 10.1148/radiol.232298 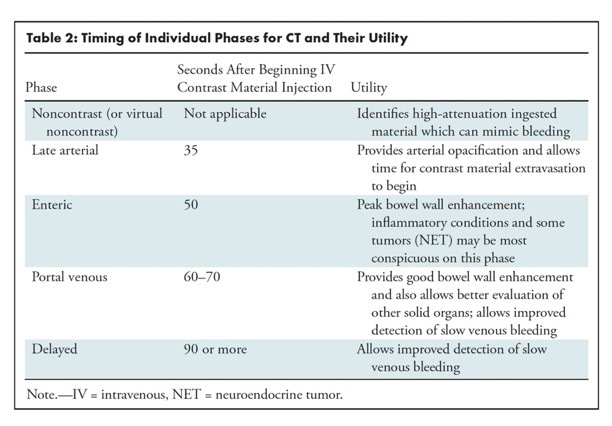
The Role of Imaging for GI Bleeding: ACG and SAR Consensus Recommendations.
Sengupta N,et al.
Radiology. 2024 Mar;310(3):e232298. doi: 10.1148/radiol.232298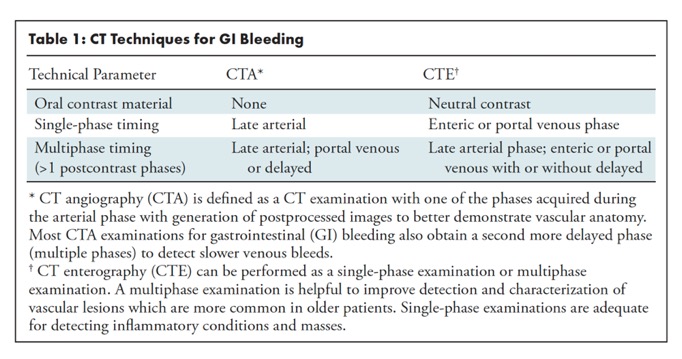
The Role of Imaging for GI Bleeding: ACG and SAR Consensus Recommendations.
Sengupta N,et al.
Radiology. 2024 Mar;310(3):e232298. doi: 10.1148/radiol.232298- “Because of its noninvasive nature, short examination time, and widespread availability, CTA is well-suited to evaluate patients with overt GI bleeding, particularly in hemodynamically unstable patients. In patients with overt GI bleeding, CT is used to identify intraluminal blood products or active contrast material extravasation to localize the site of hemorrhage and can also detect etiologies outside of the GI tract. CT techniques such as digital subtraction and dual-energy acquisition have improved the ability of CT to detect subtle GI tract lesions . CTA also provides additional information regarding the patient’s vascular and enteric anatomy, which is often helpful for choosing and planning a subsequent interventional radiology, endoscopic, or surgical procedure.”
The Role of Imaging for GI Bleeding: ACG and SAR Consensus Recommendations.
Sengupta N,et al.
Radiology. 2024 Mar;310(3):e232298. doi: 10.1148/radiol.232298 - “The biggest limitation of 99mTc-RBC scans is that this study can only be performed on hemodynamically stable patients. The RBC labeling preparation time and long imaging times prevents performing this study on patients who are hemodynamically unstable because of hypotension or abnormal heart rate. The risk-benefit ratio of obtaining a 99mTc-RBC scan, which has a long imaging time, versus correctly identifying an active LGIB site has to be weighed in borderline hemodynamically ,unstable patients.”
The Role of Imaging for GI Bleeding: ACG and SAR Consensus Recommendations.
Sengupta N,et al.
Radiology. 2024 Mar;310(3):e232298. doi: 10.1148/radiol.232298 - “CTE may have several advantages over endoscopic techniques. CTE has greater sensitivity for detecting small bowel masses, particularly those that are mural-based, and can help direct targeted, deep enteroscopy procedures when a source is identified. Cross-sectional imaging techniques (CT and MRI) allow visualization of extraintestinal abdominopelvic structures such as malignancies that may involve bowel or changes in the mesentery, bowel wall, and bowel/mesenteric vessels as potential causes of GI bleeding even in the absence of active contrast material extravasation. In patients with occult small bowel bleeding and relative contraindications to capsule endoscopy such as radiation, prior surgery, Crohn disease, and/or small bowel stenosis, CTE maybe the first-line study to characterize the abnormality .”
The Role of Imaging for GI Bleeding: ACG and SAR Consensus Recommendations.
Sengupta N,et al.
Radiology. 2024 Mar;310(3):e232298. doi: 10.1148/radiol.232298



- “In conclusion, when applied to CTs obtained to assess suspected BO, a model combining supervised 2D and 3D convolutional neural networks effectively identified those CTs showing evidence of BO. Leveraging this model has the potential to enhance the triage process for abdominal scans and therefore to appropriate patient management, notably during on-call hours. Furthermore, this approach acts as the first step in automating the selection of patients with mechanical small BO and assessing the severity of CT signs that indicate the need for surgical management.”
Deep learning for automatic bowel-obstruction identification on abdominal CT
Quentin Vanderbecq et al.
European Radiology https://doi.org/10.1007/s00330-024-10657 - Rationale and objectives: Automated evaluation of abdominal computed tomography (CT) scans should help radiologists manage their massive workloads, thereby leading to earlier diagnoses and better patient outcomes. Our objective was to develop a machine-learning model capable of reliably identifying suspected bowel obstruction (BO) on abdominal CT.
Conclusion: The 3D mixed convolutional neural network developed here shows great potential for the automated binary classification (BO yes/no) of abdominal CT scans from patients with suspected BO.
Clinical relevance statement: The 3D mixed CNN automates bowel obstruction classification, potentially automating patient selection and CT prioritization, leading to an enhanced radiologist workflow.
Deep learning for automatic bowel-obstruction identification on abdominal CT
Quentin Vanderbecq et al.
European Radiology https://doi.org/10.1007/s00330-024-10657 - Key Points
• Bowel obstruction’s rising incidence strains radiologists. AI can aid urgent CT readings.
• Employed 1345 CT scans, neural networks for bowel obstruction detection, achieving high accuracy and sensitivity on external testing.
• 3D mixed CNN automates CT reading prioritization effectively and speeds up bowel obstruction diagnosis.
Deep learning for automatic bowel-obstruction identification on abdominal CT
Quentin Vanderbecq et al.
European Radiology https://doi.org/10.1007/s00330-024-10657 - “In conclusion, when applied to CTs obtained to assess suspected BO, a model combining supervised 2D and 3D convolutional neural networks effectively identified those CTs showing evidence of BO. Leveraging this model has the potential to enhance the triage process for abdominal scans and therefore to appropriate patient management, notably during on-call hours. Furthermore, this approach acts as the first step in automating the selection of patients with mechanical small BO and assessing the severity of CT signs that indicate the need for surgical management.”
Deep learning for automatic bowel-obstruction identification on abdominal CT
Quentin Vanderbecq et al.
European Radiology https://doi.org/10.1007/s00330-024-10657
Trauma
- “Owing to the development of radiomics, CT and MRI can now be used as predictive tools to better estimate response to treatment. Although major advances have been made in abdominal cancer imaging with promising results, these results are still at an early stage and often obtained with local algorithms. Although AI helps extract a huge number of features and classify them, there is a need to bring together all the information to use it in a more efficient way. The next step should be to investigate how all these advances can be implemented in the real-life setting and how they can positively influence care and outcomes in patients with abdominal cancers .State of the art imaging is forcing radiologists to rethink what they do and how they should do it. Current challenges to implementation include reimbursement issues and well-designed translational trials for AI validation that need large volumes of high-quality and representative data for the development of robust AI algorithms.”
CT and MRI of abdominal cancers: current trends and perspectives in the era of radiomics and artificial intelligence
Maxime Barat · Anna Pellat · Christine Hoeffel · Anthony Dohan · Romain Coriat · Elliot K. Fishman · Stéphanie Nougaret · Linda Chu · Philippe Soyer
Japanese Journal of Radiology (2024) 42:246–260 - The radiologic finding of focal stenosis of the main pancreatic duct is highly suggestive of pancreatic cancer. Even in the absence of a mass lesion, focal duct stenosis can lead to surgical resection of the affected portion of the pancreas. We present four patients with distinctive pathology associated with non-neoplastic focal stenosis of the main pancreatic duct. The pathology included stenosis of the pancreatic duct accompanied by wavy, acellular, serpentine-like fibrosis, chronic inflammation with foreign body–type giant cell reaction, and calcifications. In all cases, the pancreas toward the tail of the gland had obstructive changes including acinar drop-out and interlobular and intralobular fibrosis. Three of the four patients had a remote history of major motor vehicle accidents associated with severe abdominal trauma. These results emphasize that blunt trauma can injure the pancreas and that this injury can result in long term complications, including focal stenosis of the main pancreatic duct. Pathologists should be aware of the distinct pathology associated with remote trauma and, when the pathology is present, should elicit the appropriate clinical history.
Distinctive Pathology Associated With Focal Stenosis of the Main Pancreatic Duct Secondary to Remote Trauma: A Long-term Complication of Seat Belt Pancreatitis.
Wu AA, Thompson ED, Cameron JL, He J, Burkhart RA, Burns WR, Lafaro KJ, Shubert CR, Canto MI, Fishman EK, Hruban RH.
Am J Surg Pathol. 2024 Mar 14. doi: 10.1097/PAS.0000000000002207. Epub ahead of print. PMID: 38482693. - The radiologic finding of focal stenosis of the main pancreatic duct is highly suggestive of pancreatic cancer. Even in the absence of a mass lesion, focal duct stenosis can lead to surgical resection of the affected portion of the pancreas. We present four patients with distinctive pathology associated with non-neoplastic focal stenosis of the main pancreatic duct. The pathology included stenosis of the pancreatic duct accompanied by wavy, acellular, serpentine-like fibrosis, chronic inflammation with foreign body–type giant cell reaction, and calcifications. In all cases, the pancreas toward the tail of the gland had obstructive changes including acinar drop-out and interlobular and intralobular fibrosis. Three of the four patients had a remote history of major motor vehicle accidents associated with severe abdominal trauma. These results emphasize that blunt trauma can injure the pancreas and that this injury can result in long term complications, including focal stenosis of the main pancreatic duct. Pathologists should be aware of the distinct pathology associated with remote trauma and, when the pathology is present, should elicit the appropriate clinical history.
Distinctive Pathology Associated With Focal Stenosis of the Main Pancreatic Duct Secondary to Remote Trauma : A Long-term Complication of Seat Belt Pancreatitis Annie A.
Wu, MD, PhD,* Elizabeth D. Thompson, MD, PhD,*† John L. Cameron, MD,‡ Jin He, MD, PhD,‡ Richard A. Burkhart, MD,‡ William R. Burns, MD,‡ Kelly J. Lafaro, MD, MPH,‡ Christopher R. Shubert, MD, MHA,‡ Marcia I. Canto, MD, MHS,†§ Elliot K. Fishman, MD,∥ and Ralph H. Hruban, MD*†
Am J Surg Pathol 2024;00:000–000) (in press) - “Four cases of non-neoplastic cutoff of the main pancreatic duct with distinctive pathology are presented. The pathology included abrupt duct stenosis, changes suggestive of rupture of the pancreatic duct, wavy, acellular, serpentine-like stromal fibrosis, and a foreign body– type giant cell reaction. IgG4 immunohistochemical stain was below the threshold in all cases, ruling out a type 1 autoimmune pancreatitis, and no neoplasms were present. Three of the four patients had a history of major motor vehicle accidents with associated severe abdominal trauma, suggesting that the unique pathology was caused by the trauma.”
Distinctive Pathology Associated With Focal Stenosis of the Main Pancreatic Duct Secondary to Remote Trauma : A Long-term Complication of Seat Belt Pancreatitis Annie A.
Wu, MD, PhD,* Elizabeth D. Thompson, MD, PhD,*† John L. Cameron, MD,‡ Jin He, MD, PhD,‡ Richard A. Burkhart, MD,‡ William R. Burns, MD,‡ Kelly J. Lafaro, MD, MPH,‡ Christopher R. Shubert, MD, MHA,‡ Marcia I. Canto, MD, MHS,†§ Elliot K. Fishman, MD,∥ and Ralph H. Hruban, MD*†
Am J Surg Pathol 2024;00:000–000) (in press)