Balancing Diagnostic Efficacy and Radiation Modulation for MDCT Imaging of Renal Cell CarcinomaBalancing Diagnostic Efficacy and Radiation Modulation for MDCT Imaging of Renal Cell Carcinoma Elliot K Fishman, MD, FACR The Russell H. Morgan Department of Radiology and Radiological Science The Johns Hopkins Medical Institutions Baltimore, MD |
Multiphase & MPR for Detection Subtle hypervascular lesion within the posterior right kidney, which is isoattenuating on venous phase and only apparent on the arterial images. The lesion is subtle on the axial image but is more apparent on coronal MPR. Inspection of kidneys with coronal MPRs is critical component of search patterns to ensure diagnostic efficacy. 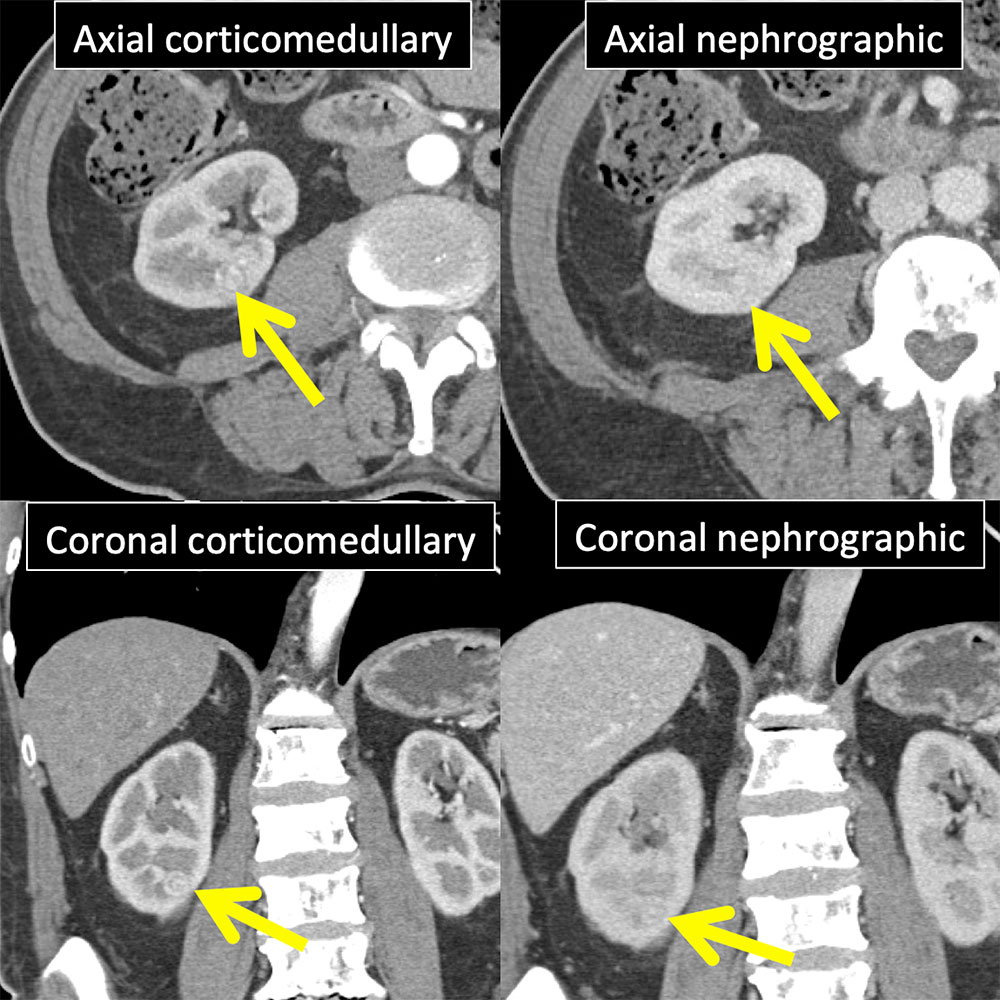 |
Clear Cell RCC Case Classic imaging features in 71 year old female with pathologically proven clear cell RCC (arrow) of the right kidney. Heterogeneous avidly enhancing lesion that is highest attenuation on arterial phase and progressively washes out measuring 160 HU on corticomedullary phase, 155 HU on nephrographic phase, and 86 HU on delayed phase. 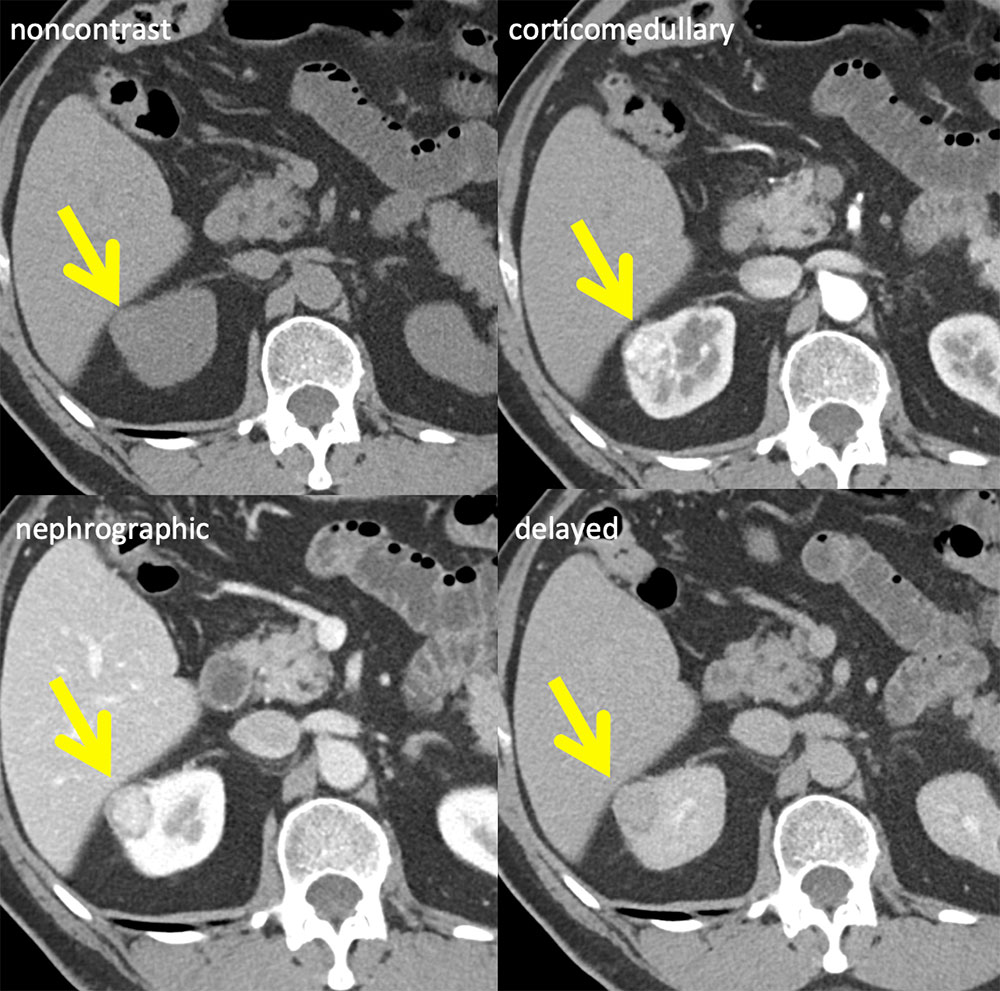 |
Papillary RCC Case Homogeneous mildly enhancing lesion within the right kidney reaching 49 HU on corticomedullary phase and 66 HU on venous and delayed phases resected and found to be a papillary RCC. Progressive enhancement as seen in this case characteristic of papillary lesions and not a feature of clear cell lesions. 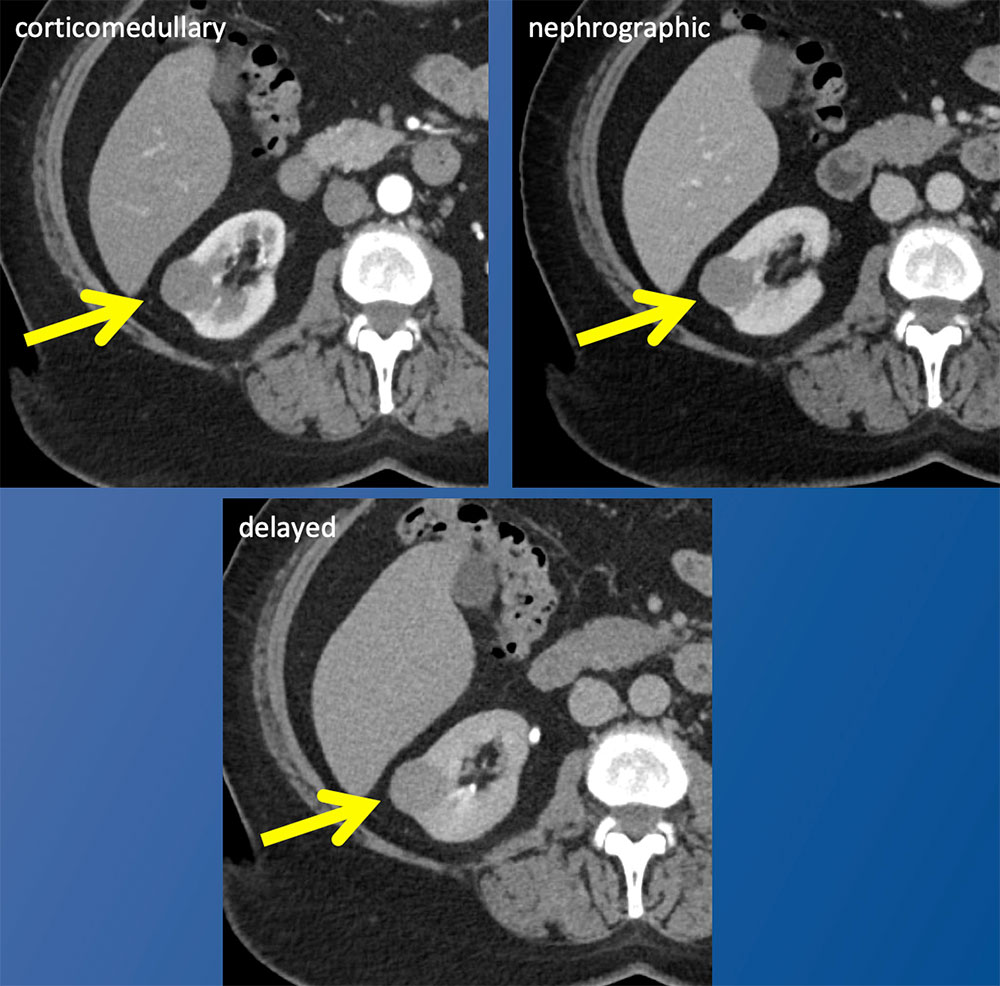 |
CT Findings Aiding in Surgical Planning 79 year old woman with newly diagnosed highly vascular clear cell carcinoma in the right kidney. Multiphase imaging enables reliable distinction of clear cell from papillary and chromophobe variants by demonstrating CM phase hypervascularity and progressive washout on nephrographic and delayed phases. Large feeding arteries (circle), demonstrated by arterial phase MIP rendering, may result in conversion from a laparoscopic to an open procedure and are important to report to the urologist. 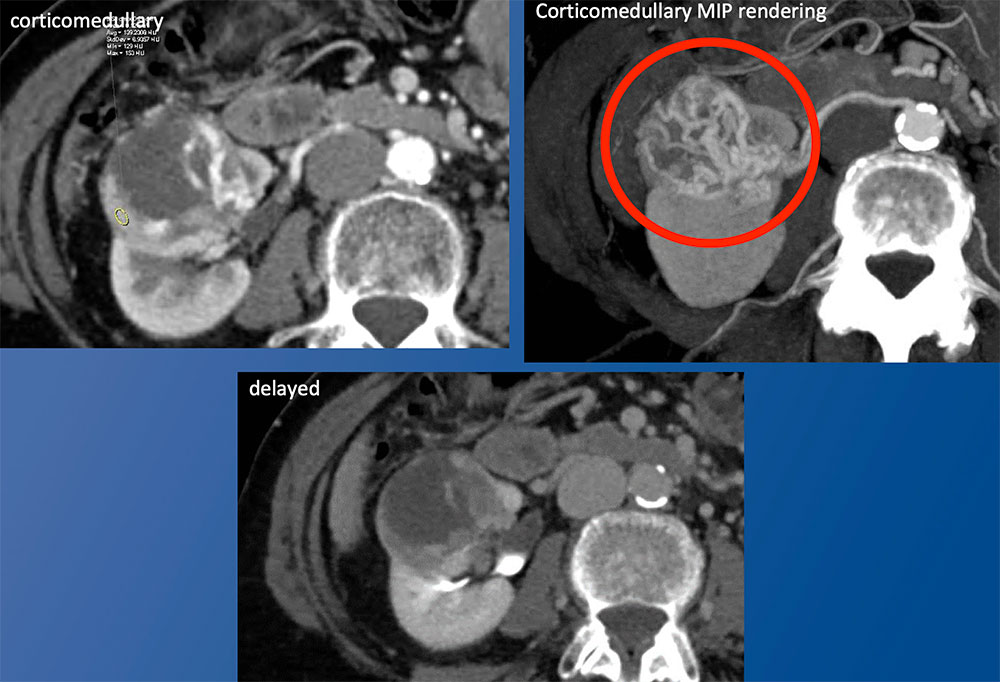 |
Partial Nephrectomy: Surgical Material vs Tumor Noncontrast images are essential in the postoperative patient to distinguish surgical material from enhancing tumor recurrence. These images demonstrate surgical material (arrow) at the nephrectomy site that mimics enhancement on postcontrast images. 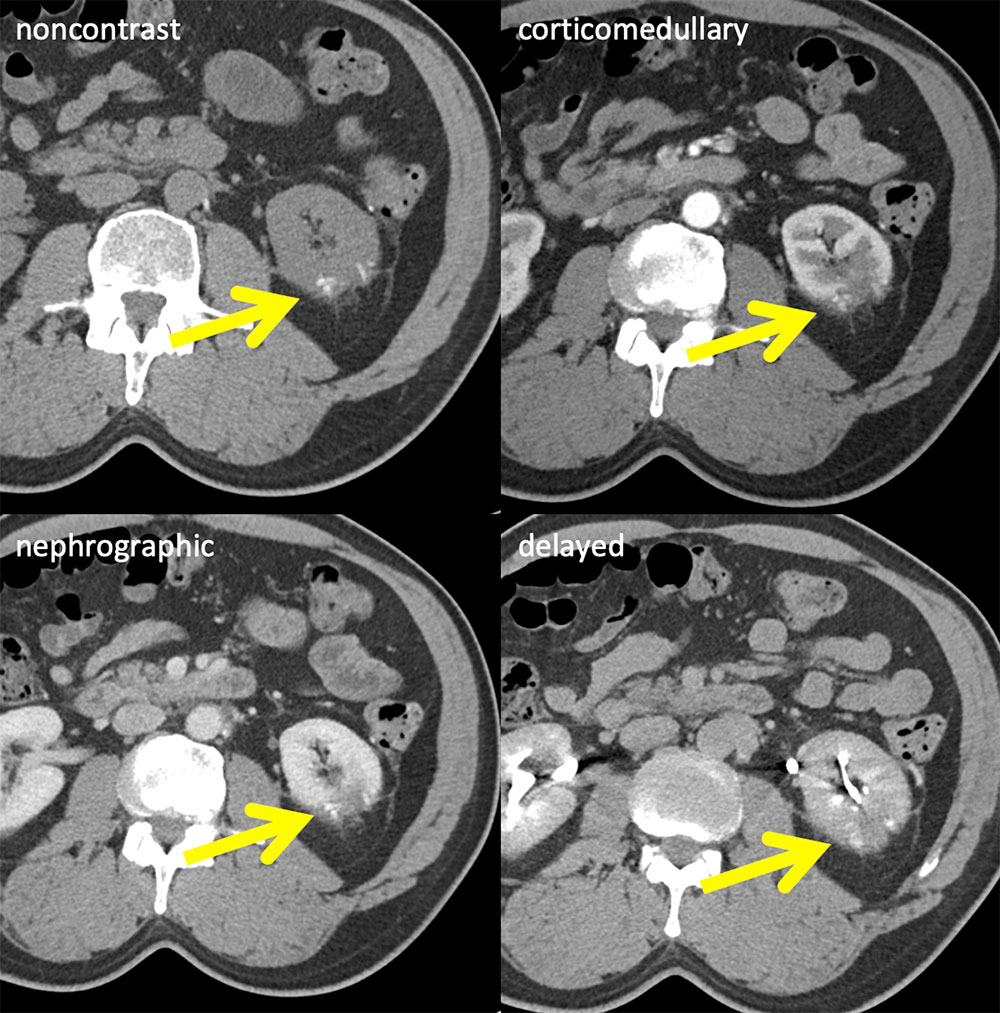 |
Partial Nephrectomy: Surgical Material vs Tumor Status post partial nephrectomy with a focus of enhancement (arrow) on corticomedullary phase representing local recurrence. Noncontrast images enable the distinction between surgical material and enhancing lesion. The recurrent lesion is isodense on venous and delayed phase, underscoring the importance of the arterial acquisition . 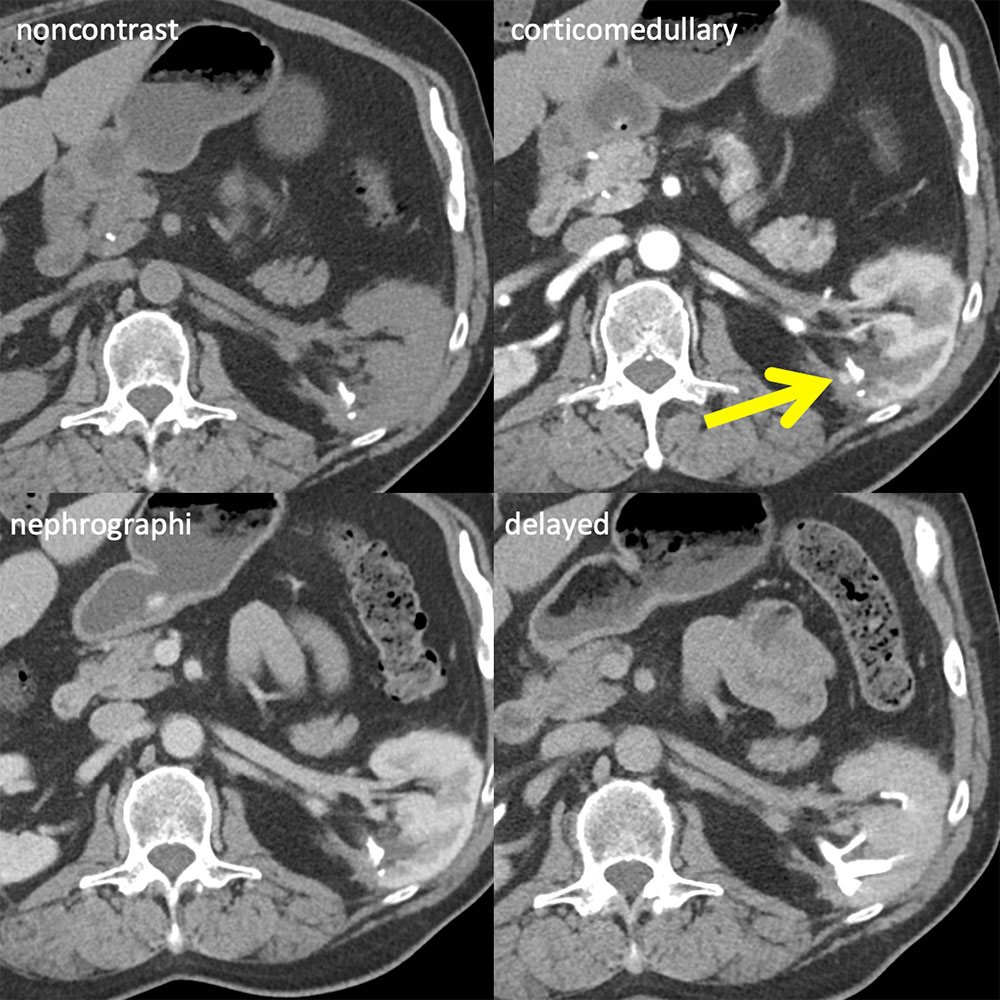 |
Pancreatic and Contralateral Kidney Metastases Patient with left clear cell RCC status post nephrectomy, metastases to the contralateral kidney (arrows) and pancreatic tail (circle). The lesions avidly enhance on arterial phase. The renal lesion is nearly isodense on each of the additional phases while the pancreatic lesion remains mildly hyperdense relative to parenchyma on the venous phase. Noncontrast is noncontributory. 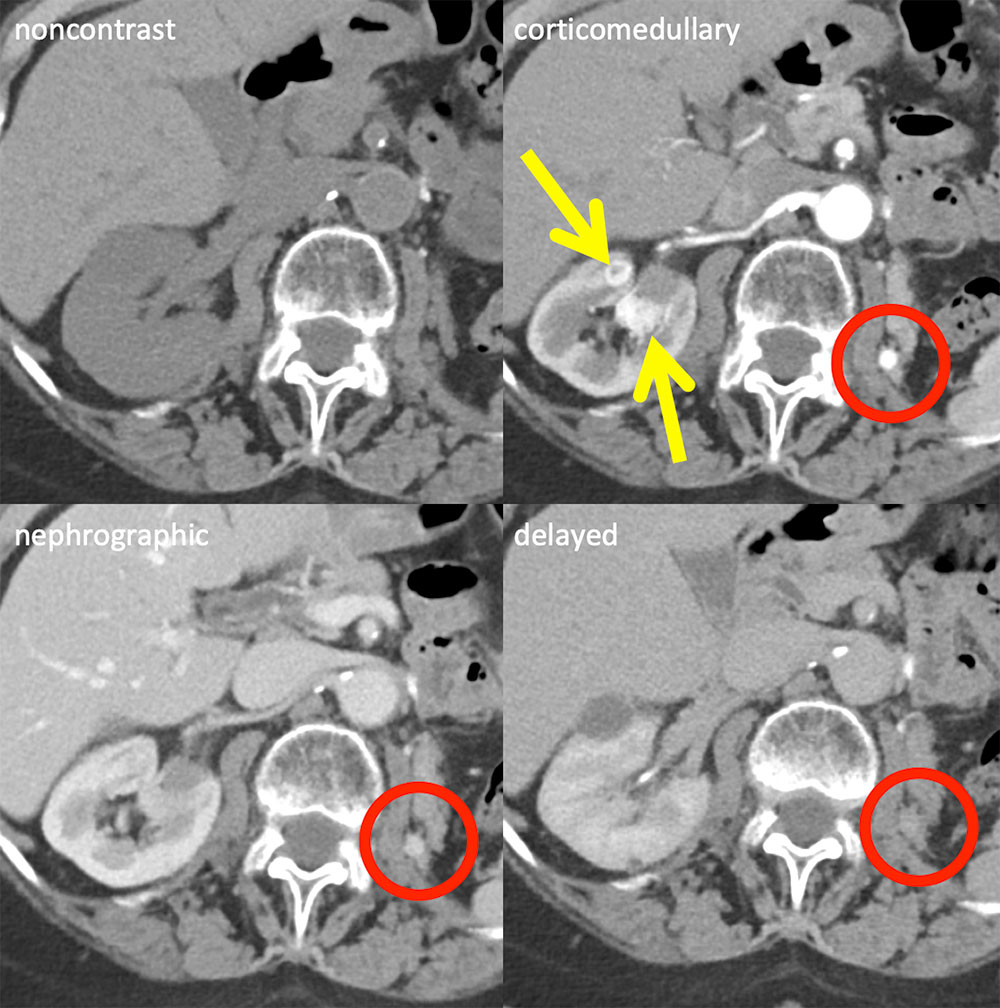 |
Clear Cell RCC Metastasis Two different patients are shown. On the left (A,B), arterial and delayed phase images in a patient with clear cell RCC show an arterial phase avidly enhancing metastatic lesion in the left seminal vesicle (circle),which would have been missed on the delayed phase. On the right (C,D), patient with clear cell status post left nephrectomy has a right paraspinal enhancing metastatic lesion (arrow) more conspicuous on arterial phase. 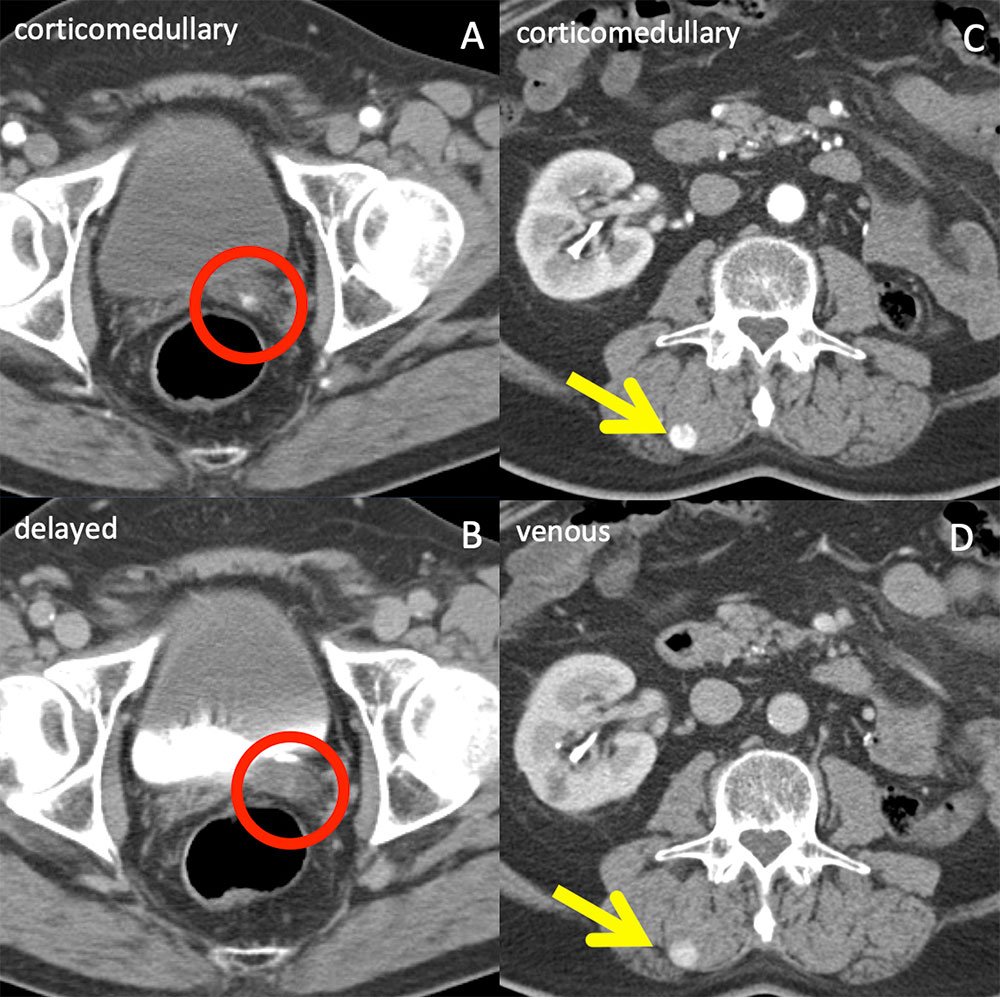 |
Pancreatic Uncinate Metastasis Status post right nephrectomy for clear cell RCC with avidly enhancing metastasis (circle) in the pancreatic uncinate only discernible on arterial phase. The lesion becomes isodense to pancreatic parenchyma on venous phase, again demonstrating the diagnostic importance of arterial phase imaging in RCC surveillance. 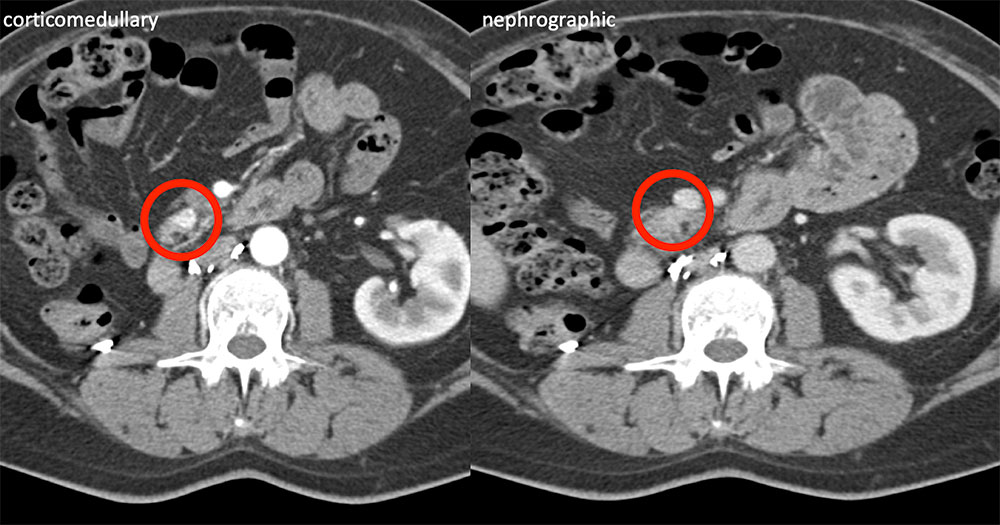 |
Hepatic Metastasis Patient with clear cell RCC status post partial left nephrectomy with avidly enhancing metastatic liver lesions (circles) seen only on arterial phase. The lesions are isodense on all other phases. This case demonstrates the importance of arterial phase imaging in renal cell carcinoma follow-up. Noncontrast is noncontributory. 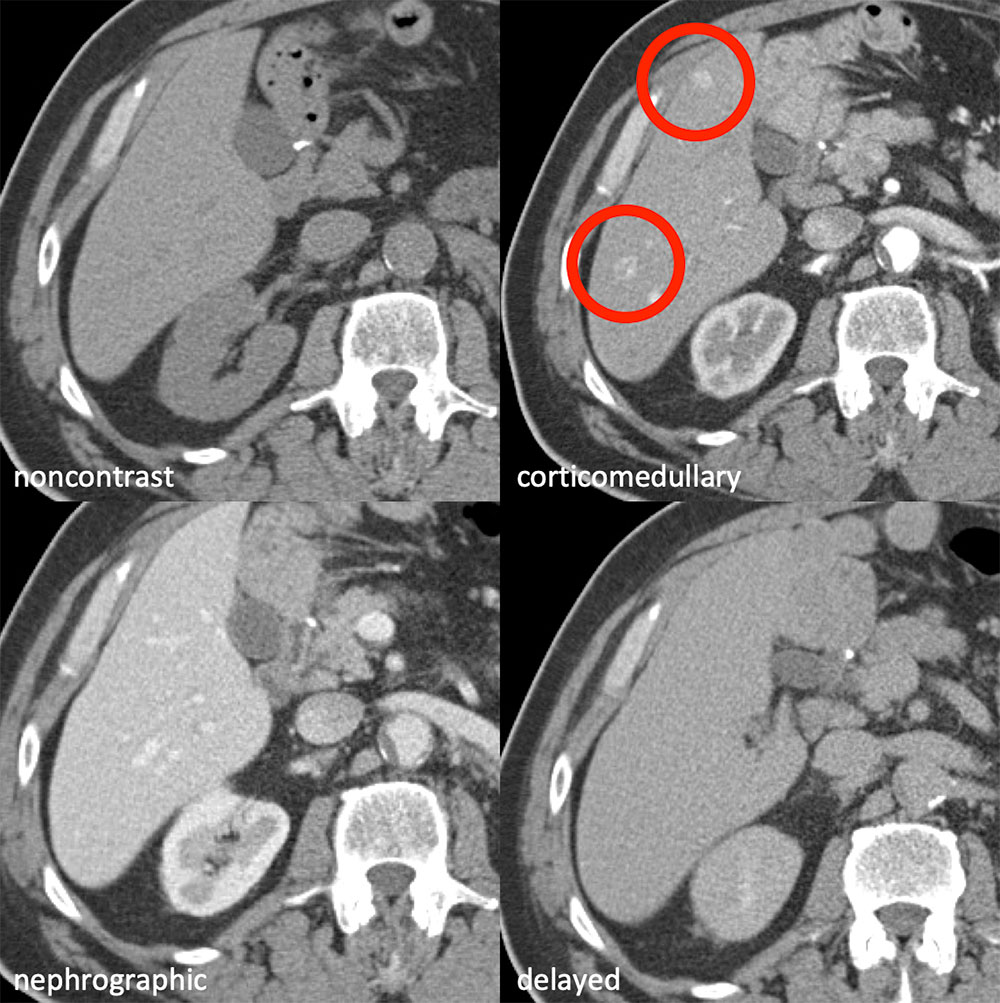 |
Contralateral Kidney Metastases 59 year old man status post left nephrectomy for renal cell carcinoma with clear cell and papillary features in remission who developed metastatic disease in the contralateral kidney. Multiple enlarging masses(circles) in the right kidney showed little difference in attenuation between corticomedullary and nephrographic or nephrographic and delayed acquisitions. Comparison across > 2 phases is required for high diagnostic confidence regarding whether the new lesion is a complex cyst or solid mass. Either precontrast or delayed should be performed in addition to corticomedullary and nephrographic. 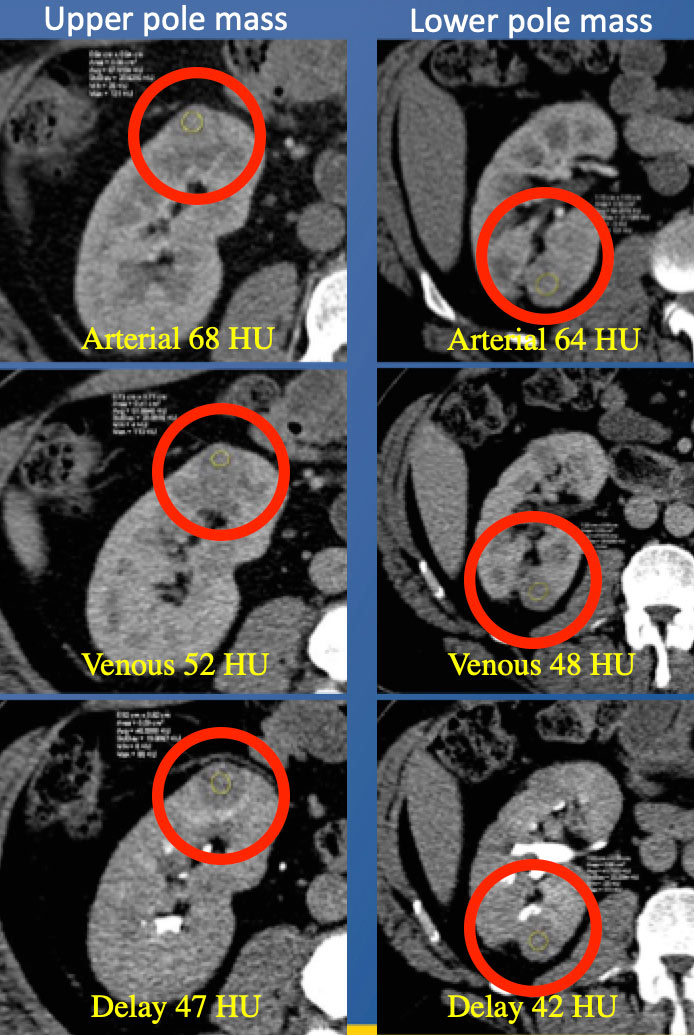 |
References
|
References
|
References
|
References
|