
Artificial Intelligence for Early Detection of Pancreatic Cancer: Preliminary Observations and Challenges
Artificial Intelligence for Early Detection of Pancreatic Cancer: Preliminary Observations and Challenges Satomi Kawamoto, M.D. The Russell H. Morgan Department of Radiology and Radiological Science, Department of Computer Science, Department of Pathology, and the Department of Cancer Research Johns Hopkins University |
Disclosure Research supported by the Lustgarten Foundation
|
Learning Objectives
|
Introduction
|
Deep Learning Applications in Cancer Imaging
|
Table of Contents
|
Deep network prediction of normal pancreas Deep learning has largely relied on supervised learning approaches, i.e., large amounts of training data that composed of input images and ground truth annotations. We collected abdominal CT data from 575 normal subjects (potential renal donors) that are used as the input for deep CNN for development of deep learning algorithms for automatic recognition of a normal pancreas. 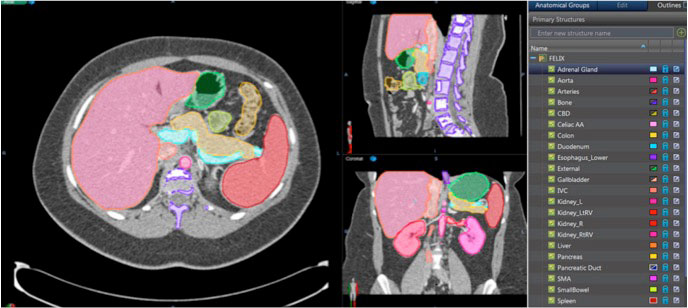 Park S, et al. Diagnostic and Interventional Imaging 2019 [Epub ahead of print] |
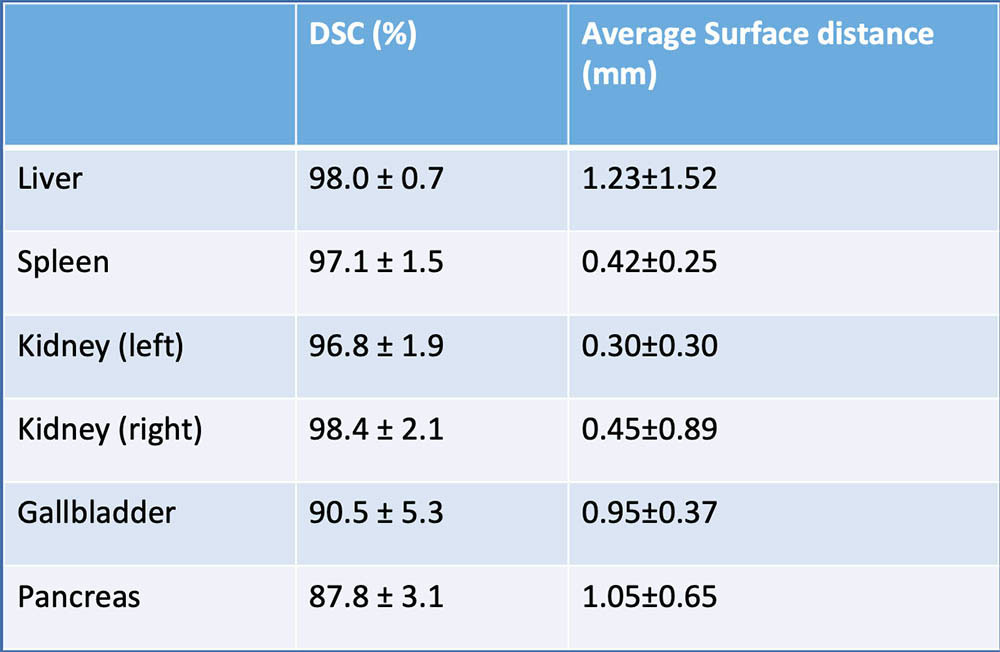
Deep network prediction of normal pancreas In our series using 236 normal CT data, deep network prediction for the pancreas showed high fidelity with mean Dice similarity coefficients of 87.8±3.1% and mean surface distances of 1.05 ± 0.65 mm. 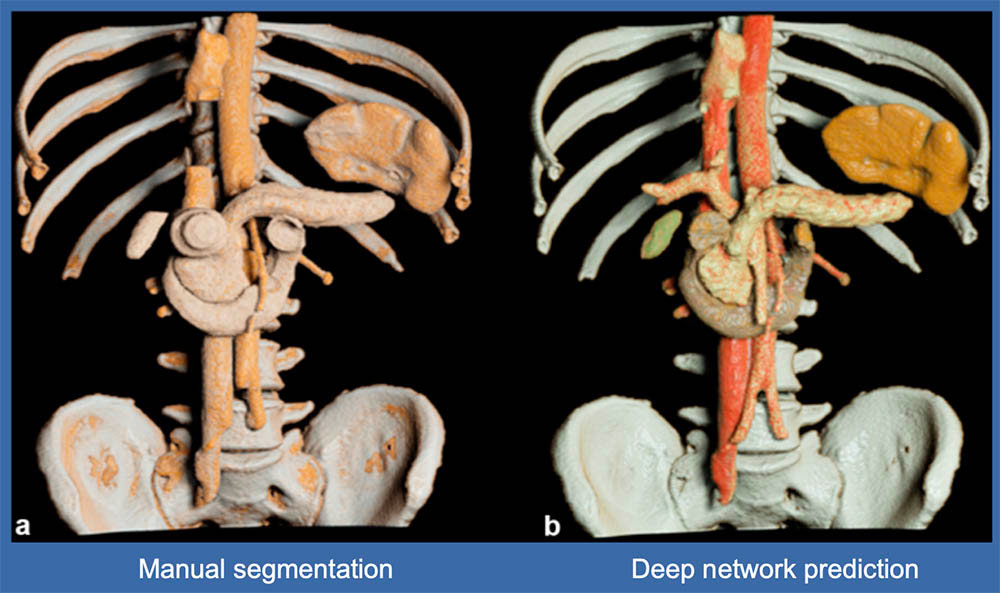 Wang Y, et al. http://arxiv.org/abs/1804.08414 Park S, et al. Diagnostic and Interventional Imaging 2019 [Epub ahead of print] |
Deep network prediction of normal pancreas and other organs
 Wang Y, et al. http://arxiv.org/abs/1804.08414 Park S, et al. Diagnostic and Interventional Imaging 2019 [Epub ahead of print] |
Deep network prediction of pancreatic cancer
 |
Deep network prediction of pancreatic cancer The proposed framework of these studies offers high sensitivity (94.1%) and specificity (98.5%), which demonstrates the potential to make a clinical impact.
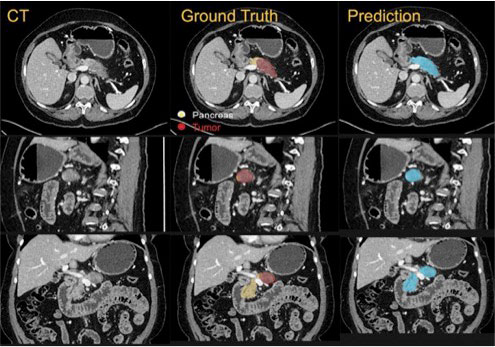 RSNA News https://www.rsna.org/news/2018/april/machine-learning-benefits-radiology |
Deep network prediction of pancreatic cancer: Difficult cases
|
Example of FALSE NEGATIVE case of deep network prediction of pancreatic cancer (PNET) Small PNET in the body of the pancreas seen as a subtle enhancing lesion in arterial phase, and nearly iso-atteunating to the normal pancreas in venous phase, but visible by precontrast T1-weighted MRI. 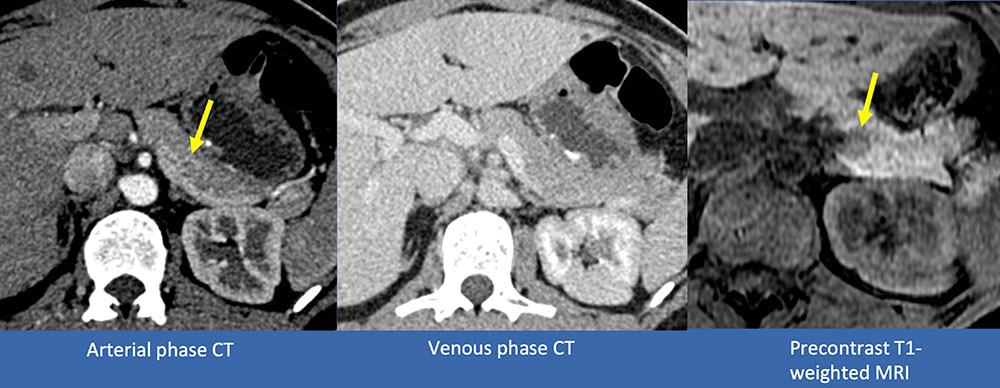 |
Example of FALSE NEGATIVE case of deep network prediction of pancreatic cancer (PNET) Small PNET in the body of the pancreas seen as a subtle enhancing lesion in arterial phase, and not visible in venous phase. 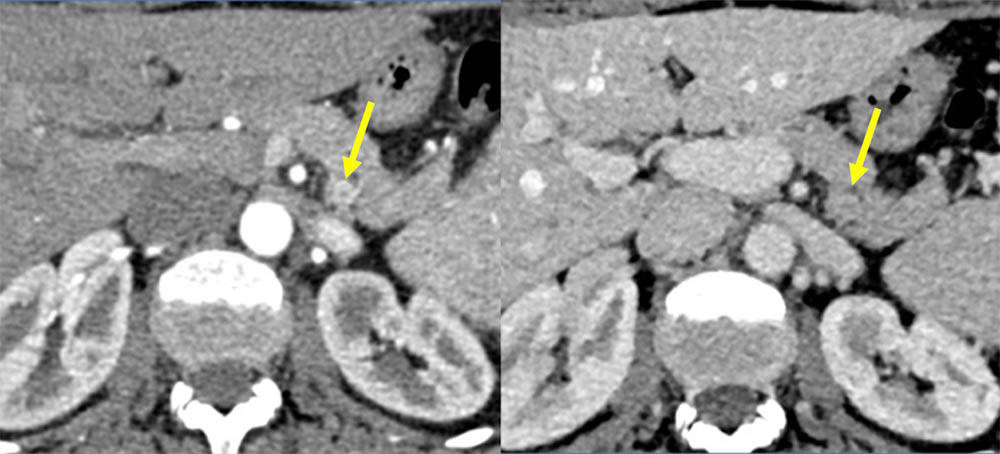 |
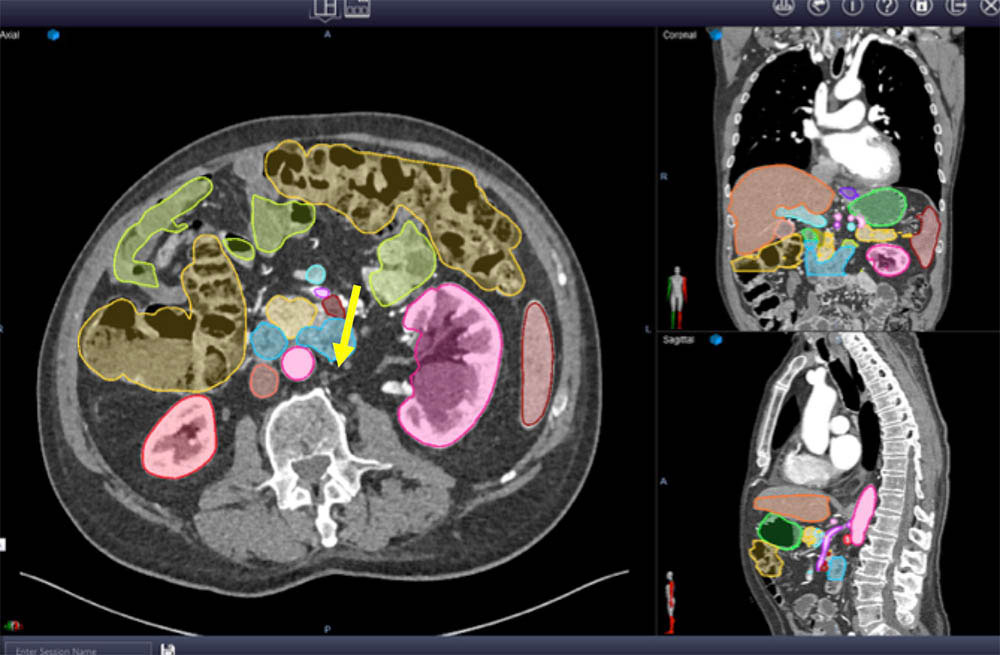
Example of FALSE NEGATIVE case of deep network prediction of pancreatic cancer (PNET) Small PNET in the body of the pancreas seen as a subtle enhancing mass (yellow arrow) in arterial phase with upstream pancreatic duct dilatation (blue arrow). 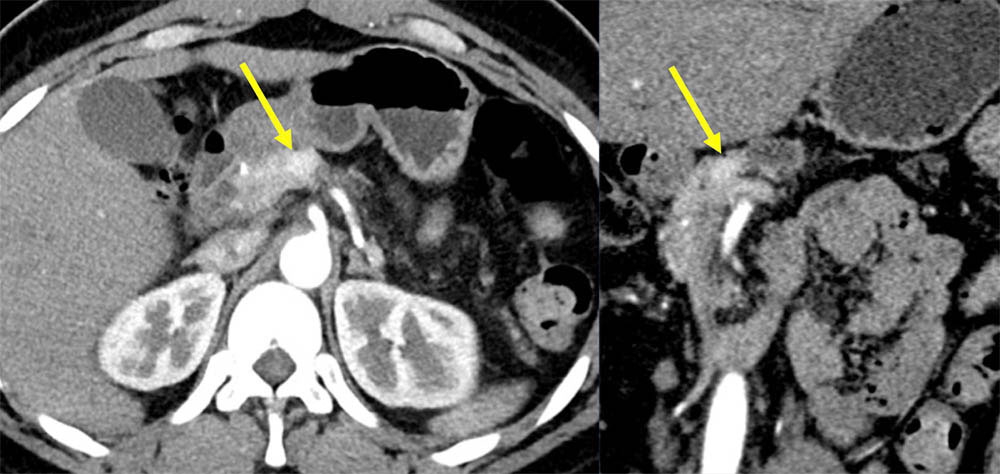 |
Example of FALSE POSITIVE case of deep network prediction of pancreatic cancer (PDAC) False positive PDAC prediction in the head of the pancreas Uneven focal fatty infiltration of the head of the pancreas might be related to false positive prediction 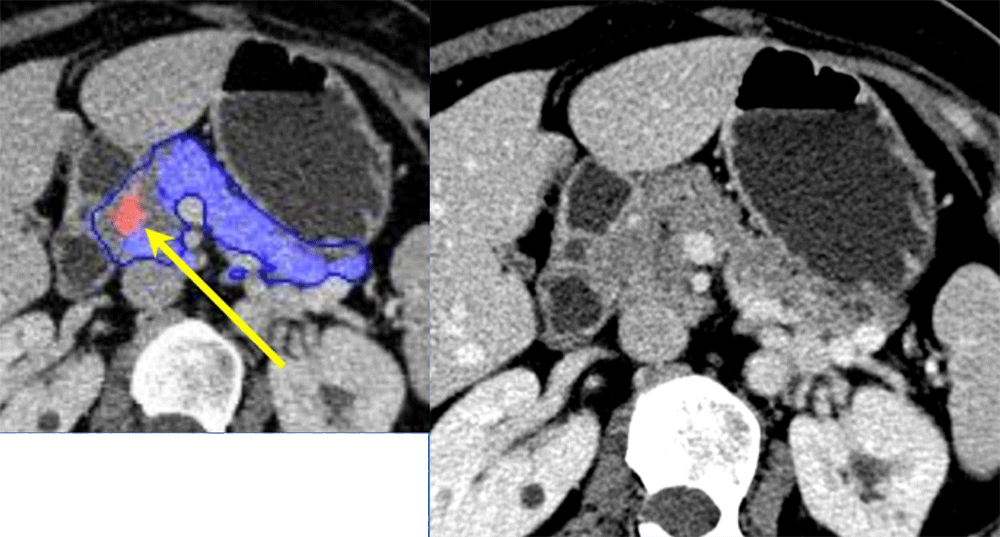 Wang Y, Zhou Y, Shen W, Park S, Fishman EK, Yuille AL. Abdominal multi-organ segmentation with organ-attention networks and statistical fusion. https://arxiv.org/abs/1804.08414 |
Example of FALSE POSITIVE case of deep network prediction of pancreatic cancer (PDAC) False positive PDAC prediction in the head of the pancreas Uneven focal fatty infiltration of the head of the pancreas might be related to false positive prediction 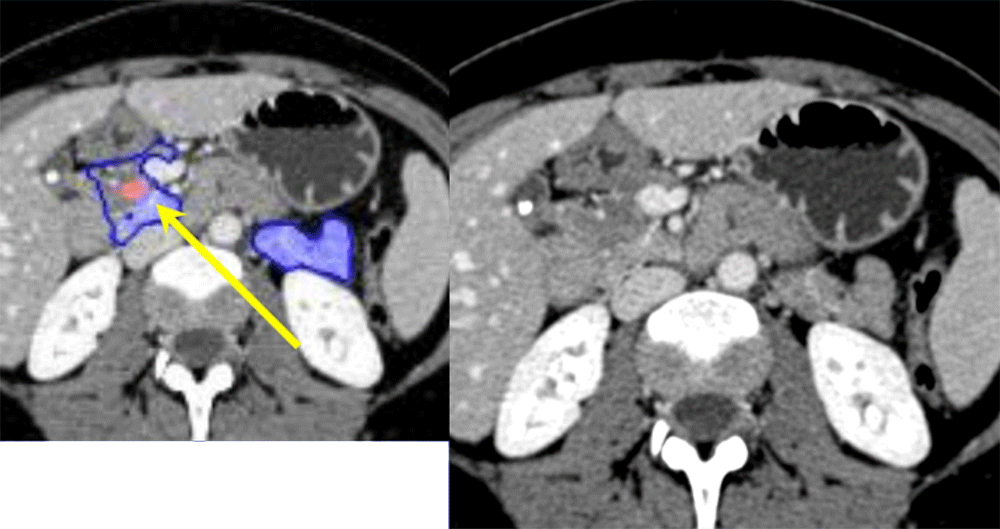 Wang Y, Zhou Y, Shen W, Park S, Fishman EK, Yuille AL. Abdominal multi-organ segmentation with organ-attention networks and statistical fusion. https://arxiv.org/abs/1804.08414 |
Challenges in detection of pancreatic cancer
|
Challenges in obtaining large training data
|
Challenges in increasing training data
|
Challenges in data segmentation
Chu L, et al. Application of deep learning to pancreatic cancer detection lessons learned from our initial experience JACR 2019;9:1338 |
Challenges in segmentation of pancreatic cancer
|
Example of challenging PNET case for segmentation Small PNET in the body of the pancreas seen as a subtle enhancing mass seen only in arterial phase (yellow arrow), only possible with correlation with EUS finding (7 mm hypoechoic mass was detected in the anterior portion of the tail by EUS). This case was FALSE NEGATIVE by deep network prediction. 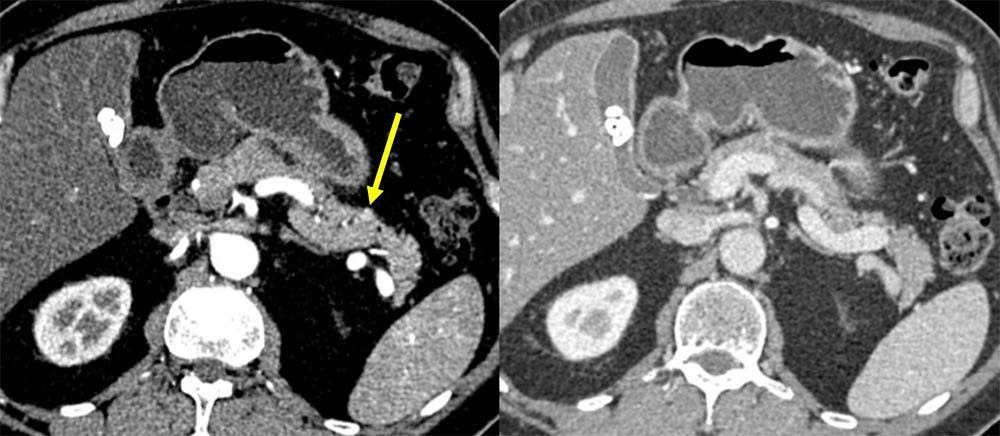 |
Potential advantages to segment other abdominal organs We decided to annotate not only pancreas but other abdominal organs because
Chu L, et al. Application of deep learning to pancreatic cancer detection lessons learned from our initial experience JACR 2019;9:1338 |
Example of advantage to segment other abdominal organs 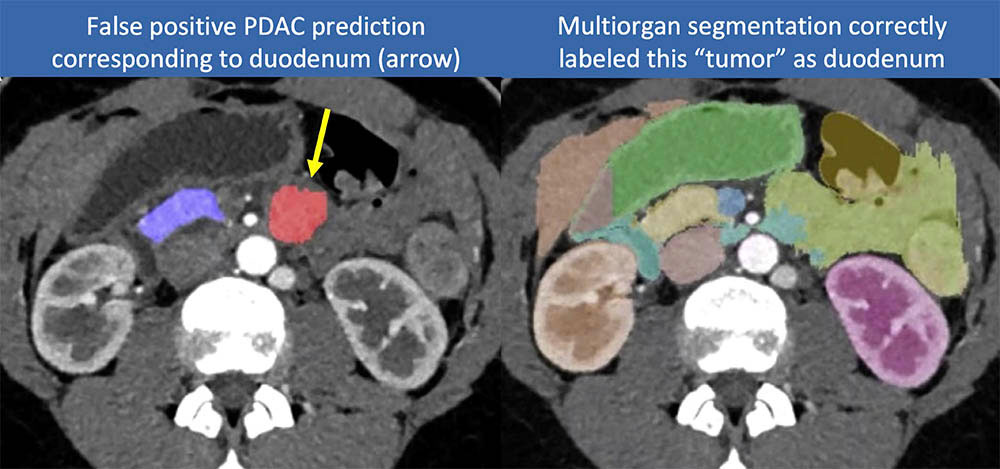 Chu L, et al. Application of deep learning to pancreatic cancer detection lessons learned from our initial experience JACR 2019;9:1338 |
Future Vision
|
Conclusion (1)
|
Conclusion (2)
|
References
Acknowledgements
|